Cervical Spine Malalignment - True or Pseudo Subluxation ?
Radiology Cases in Pediatric Emergency Medicine
Volume 1, Case 5
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
A 6 year old female was taken to a rural emergency
department with a complaint of neck pain. Her behavior
was described as slightly different. She didn't want to
walk around and she was not moving her head much.
The only history of trauma that was obtained was being
thrown into a swimming pool about 32 hours ago. She
was difficult to examine but she was noted to have
some tenderness over her posterior neck. A cervical
spine series was obtained.
View radiographs.
 AP and odontoid views were also done, but they are
not shown here. This lateral view shows a
malalignment of the vertebral bodies of C2-C3. A stiff
collar was applied, she was placed on a spine board,
and transferred to a children's hospital.
During transport, she fell asleep and the transport
took place without incident. Upon arrival, she awoke
and became very agitated despite the presence of her
mother. She complained that she couldn't breathe and
the back of her head hurt. She was moving her head
around excessively despite the immobilization
measures. The physician on duty examined the
radiographs and felt that the C2-C3 malalignment
represented a normal finding, pseudosubluxation. An
opinion with a radiologist was sought via teleradiology,
who agreed that this was a pseudosubluxation.
Because of her agitation, she was taken out of cervical
spine immobilization. The risk of cervical spine injury
was felt to be low because of the normal radiographs,
the relatively benign mechanism of injury, and her
delayed ambulatory presentation.
After the cervical spine immobilization was removed,
the examination of her neck revealed mild tenderness
on palpation of the spinous processes in the mid portion
of her neck. Range of motion was limited in all
directions and associated with some pain. It was
difficult to assess the degree of muscle spasm in her
neck. There were no complaints of paresthesia. Motor
and sensory functions were fully intact.
A CT scan of the cervical spine was obtained to rule
out rotary subluxation given her unwillingness to move
her neck. This study was normal. Her behavior
appeared to normalize and she was ambulating well.
Her neck symptoms persisted. She was discharged
from the emergency department. She recovered
spontaneously without any complications.
Teaching Points:
Rotary subluxation of one of the cervical spine
elements (usually C1-C2) can be a difficult diagnosis to
make. Plain films are often difficult to interpret. The
patient may present with torticollis, which is usually due
to benign muscle spasm often following a viral infection.
Although most patients with torticollis do not have rotary
subluxation, the task of deciding whom to evaluate
further is difficult. CT scanning the cervical spine can
more definitively assess the rotational relationships of
the cervical spine elements and more effectively rule
out rotary subluxation.
Developmental variants of the cervical spine in
young children can be difficult to deal with when
interpreting radiographs using measurement
parameters based on adults.
The space between the atlas and the odontoid can
be 4 to 5 mm in children up to age 15 years, compared
to 2 mm for adults. This is because the odontoid is not
fully ossified. The radiograph shows only the ossified
core, while the outer layers of the odontoid are still
cartilaginous and not visible on radiographs.
Depending on the positioning of the child's neck, it is
not unusual to see a straight cervical spine on the
lateral view without the usual lordosis. In adults, the
absence of lordosis is an indirect sign of muscle spasm,
possibly due to an occult fracture. However, in
children, the absence of lordosis is not indicative of
muscle spasm.
In children up to age 10 years, flexion and extension
are greatest about C2 and C3. C2 may appear to be
anterior relative to C3 by as much as 5 mm. This
pseudosubluxation is increased if the radiograph is
taken with the neck flexed. This finding may be present
in as many as one-third of all lateral cervical spine films
in children.
It is extremely important to distinguish true
subluxation from pseudosubluxation. It would be
unwise to assume the presence of pseudosubluxation
until this is certain. This pseudosubluxation
phenomenon may result in a delay in establishing the
diagnosis of a true subluxation. Such patients should
be treated conservatively with cervical spine
immobilization until the true diagnosis has been
ascertained.
The two most common causes of C2-C3
malalignment are pseudosubluxation and a hangman's
fracture. To distinguish these two, Swischuk defined a
posterior cervical line drawn from the cortex of the
posterior arch of C1 to the cortex of the posterior arch
of C3. This line should pass through or be less than
1 mm anterior to the posterior arch of C2. If this
distance is greater than 1 mm (possibly up to 1.5 or 2
mm may be normal), this indicates a fracture of the
arch of C2 (The vertebral body moves anteriorly, while
the arch and the spinous process move posteriorly).
Additionally, pseudosubluxations are most
pronounced with the neck flexed. C2/C3 malalignment
should not persist if the neck is placed in a more neutral
or extended position. Persistence of the subluxation in
extension is felt to be due to injury (non-physiologic).
Determine the Swischuk line for our patient.
Our original patient's radiograph is below:
Locate the posterior arch of C1 and the posterior
arch of C3. Draw a line through this. Does this line
pass within 1 mm of the posterior arch of C2 ? The
actual dimensions on your screen are enlarged
depending on the degree of magnification and the size
of your monitor so you cannot actually measure it with a
ruler.
View the Swischuk line.
AP and odontoid views were also done, but they are
not shown here. This lateral view shows a
malalignment of the vertebral bodies of C2-C3. A stiff
collar was applied, she was placed on a spine board,
and transferred to a children's hospital.
During transport, she fell asleep and the transport
took place without incident. Upon arrival, she awoke
and became very agitated despite the presence of her
mother. She complained that she couldn't breathe and
the back of her head hurt. She was moving her head
around excessively despite the immobilization
measures. The physician on duty examined the
radiographs and felt that the C2-C3 malalignment
represented a normal finding, pseudosubluxation. An
opinion with a radiologist was sought via teleradiology,
who agreed that this was a pseudosubluxation.
Because of her agitation, she was taken out of cervical
spine immobilization. The risk of cervical spine injury
was felt to be low because of the normal radiographs,
the relatively benign mechanism of injury, and her
delayed ambulatory presentation.
After the cervical spine immobilization was removed,
the examination of her neck revealed mild tenderness
on palpation of the spinous processes in the mid portion
of her neck. Range of motion was limited in all
directions and associated with some pain. It was
difficult to assess the degree of muscle spasm in her
neck. There were no complaints of paresthesia. Motor
and sensory functions were fully intact.
A CT scan of the cervical spine was obtained to rule
out rotary subluxation given her unwillingness to move
her neck. This study was normal. Her behavior
appeared to normalize and she was ambulating well.
Her neck symptoms persisted. She was discharged
from the emergency department. She recovered
spontaneously without any complications.
Teaching Points:
Rotary subluxation of one of the cervical spine
elements (usually C1-C2) can be a difficult diagnosis to
make. Plain films are often difficult to interpret. The
patient may present with torticollis, which is usually due
to benign muscle spasm often following a viral infection.
Although most patients with torticollis do not have rotary
subluxation, the task of deciding whom to evaluate
further is difficult. CT scanning the cervical spine can
more definitively assess the rotational relationships of
the cervical spine elements and more effectively rule
out rotary subluxation.
Developmental variants of the cervical spine in
young children can be difficult to deal with when
interpreting radiographs using measurement
parameters based on adults.
The space between the atlas and the odontoid can
be 4 to 5 mm in children up to age 15 years, compared
to 2 mm for adults. This is because the odontoid is not
fully ossified. The radiograph shows only the ossified
core, while the outer layers of the odontoid are still
cartilaginous and not visible on radiographs.
Depending on the positioning of the child's neck, it is
not unusual to see a straight cervical spine on the
lateral view without the usual lordosis. In adults, the
absence of lordosis is an indirect sign of muscle spasm,
possibly due to an occult fracture. However, in
children, the absence of lordosis is not indicative of
muscle spasm.
In children up to age 10 years, flexion and extension
are greatest about C2 and C3. C2 may appear to be
anterior relative to C3 by as much as 5 mm. This
pseudosubluxation is increased if the radiograph is
taken with the neck flexed. This finding may be present
in as many as one-third of all lateral cervical spine films
in children.
It is extremely important to distinguish true
subluxation from pseudosubluxation. It would be
unwise to assume the presence of pseudosubluxation
until this is certain. This pseudosubluxation
phenomenon may result in a delay in establishing the
diagnosis of a true subluxation. Such patients should
be treated conservatively with cervical spine
immobilization until the true diagnosis has been
ascertained.
The two most common causes of C2-C3
malalignment are pseudosubluxation and a hangman's
fracture. To distinguish these two, Swischuk defined a
posterior cervical line drawn from the cortex of the
posterior arch of C1 to the cortex of the posterior arch
of C3. This line should pass through or be less than
1 mm anterior to the posterior arch of C2. If this
distance is greater than 1 mm (possibly up to 1.5 or 2
mm may be normal), this indicates a fracture of the
arch of C2 (The vertebral body moves anteriorly, while
the arch and the spinous process move posteriorly).
Additionally, pseudosubluxations are most
pronounced with the neck flexed. C2/C3 malalignment
should not persist if the neck is placed in a more neutral
or extended position. Persistence of the subluxation in
extension is felt to be due to injury (non-physiologic).
Determine the Swischuk line for our patient.
Our original patient's radiograph is below:
Locate the posterior arch of C1 and the posterior
arch of C3. Draw a line through this. Does this line
pass within 1 mm of the posterior arch of C2 ? The
actual dimensions on your screen are enlarged
depending on the degree of magnification and the size
of your monitor so you cannot actually measure it with a
ruler.
View the Swischuk line.
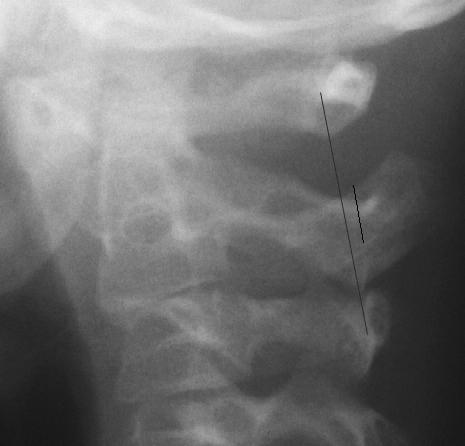 The Swischuk line is drawn on our patient's
radiograph. The posterior arch of C2 is pointed out;
however, in this example, the posterior arch of C2 is
poorly identified because the radiograph's angle is
slightly oblique. The distance from the Swischuk line to
the posterior arch of C2 is about 1.6 mm. This is more
than the 1 mm upper normal limit described by
Swischuk; however, other reports have indicated that
this distance can be up to 1.5 or 2 mm. Note that this
radiograph is taken with the neck in flexion [Click on
Neck to see flexion angle]. This artificially amplifies the
degree of C2/C3 pseudosubluxation. Ideally, the
radiograph should be taken in a neutral or extended
position to minimize the C2/C3 pseudosubluxation.
View another example.
The Swischuk line is drawn on our patient's
radiograph. The posterior arch of C2 is pointed out;
however, in this example, the posterior arch of C2 is
poorly identified because the radiograph's angle is
slightly oblique. The distance from the Swischuk line to
the posterior arch of C2 is about 1.6 mm. This is more
than the 1 mm upper normal limit described by
Swischuk; however, other reports have indicated that
this distance can be up to 1.5 or 2 mm. Note that this
radiograph is taken with the neck in flexion [Click on
Neck to see flexion angle]. This artificially amplifies the
degree of C2/C3 pseudosubluxation. Ideally, the
radiograph should be taken in a neutral or extended
position to minimize the C2/C3 pseudosubluxation.
View another example.
 This radiograph again shows a malalignment of C2
on C3. Note that again, the neck is positioned in
flexion. Is this a pseudosubluxation or a true
subluxation? Identify the posterior arches of C1 and
C3. Draw a line connecting these points. Does this line
pass within 1 mm of the posterior arch of C2 ?
Drawing the Swischuk line on this radiograph is
easier. The posterior arches of C1, C2, and C3 are well
defined.
This radiograph again shows a malalignment of C2
on C3. Note that again, the neck is positioned in
flexion. Is this a pseudosubluxation or a true
subluxation? Identify the posterior arches of C1 and
C3. Draw a line connecting these points. Does this line
pass within 1 mm of the posterior arch of C2 ?
Drawing the Swischuk line on this radiograph is
easier. The posterior arches of C1, C2, and C3 are well
defined.
 This Swischuk line intersects the posterior arch of
C2. It indicates good alignment of this region despite
the apparent malalignment of the vertebral bodies.
You should be confident that you can identify the
landmarks necessary to draw the Swischuk line. This is
important in distinguishing pseudosubluxation from a
true subluxation. Pseudosubluxation occurs commonly
(up to 33%); therefore, it is very likely that you will need
to draw the Swischuk line several times a day.
View another example.
This Swischuk line intersects the posterior arch of
C2. It indicates good alignment of this region despite
the apparent malalignment of the vertebral bodies.
You should be confident that you can identify the
landmarks necessary to draw the Swischuk line. This is
important in distinguishing pseudosubluxation from a
true subluxation. Pseudosubluxation occurs commonly
(up to 33%); therefore, it is very likely that you will need
to draw the Swischuk line several times a day.
View another example.
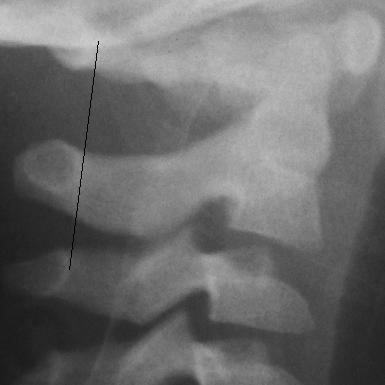
 This radiograph also shows malalignment of C2 on
C3. It again shows modest flexion. Draw the Swischuk
line on this radiograph. Drawing the Swischuk line on
this radiograph is considerably more difficult because
the posterior arch of C1 is not as obvious. The arch of
C1 is positioned obliquely in this film, thus you can
actually see the arch (it resembles a loop).
This radiograph also shows malalignment of C2 on
C3. It again shows modest flexion. Draw the Swischuk
line on this radiograph. Drawing the Swischuk line on
this radiograph is considerably more difficult because
the posterior arch of C1 is not as obvious. The arch of
C1 is positioned obliquely in this film, thus you can
actually see the arch (it resembles a loop).
 The gap between the Swischuk line and the
posterior arch of C2 is about 1 mm. This is at the upper
normal limit described by Swischuk, but other reports
have indicated that this can be up to 1.5 or 2 mm.
View this radiograph again.
This radiograph was taken as part of a foreign body
series in a patient with a bronchial foreign body. There
was no suspicion of cervical spine injury. Note that the
neck is flexed. This amplifies the C2/C3
pseudosubluxation. Neck flexion also increases the
width of the prevertebral soft tissues. In a properly
positioned radiograph, the prevertebral soft tissue
thickness should be about half the width of the vertebral
bodies (as demonstrated in the two previous
radiographs:
If this space is widened, it suggests the presence of
a retropharyngeal abscess in a febrile patient with upper
airway symptoms or soft tissue edema or bleeding from
an occult cervical spine fracture in a trauma patient. In
the [Neck-3] radiograph, the prevertebral soft tissues
are excessively wide, but not because of an abscess or
bleeding. This finding is purely due to positioning in this
case. In this case, taking the radiograph with the neck
extended will probably "cure" the patient of the
pseudosubluxation and the prevertebral soft tissue
widening.
References
Fassier F. C1-C4 Fractures and Dislocations. In:
Letts RM (ed). Management of Pediatric Fractures.
New York, Churchill Livingstone, 1994, pp. 807-831.
Ozonoff MB. The Spine. In: Ozonoff MB. Pediatric
Orthopedic Radiology. Philadelpha, W.B. Saunders
Company, 1992, pp. 1-7.
Woodward GA. Neck Trauma. In: Fleisher GR,
Ludwig S. Texbook of Pediatric Emergency Medicine,
third edition. Baltimore, Williams & Wilkins, 1993, pp.
1124-1142.
Swischuk LE. Anterior Displacement of C2 in
Children: Physiologic or Pathologic? A Helpful
Differentiating Line. Radiology 1977;122:759-763.
Chung SMK. The Neck. In: Handbook of Pediatric
Orthopedics. New York, Van Nostrand Reinhold, 1986,
pp. 43-52.
The gap between the Swischuk line and the
posterior arch of C2 is about 1 mm. This is at the upper
normal limit described by Swischuk, but other reports
have indicated that this can be up to 1.5 or 2 mm.
View this radiograph again.
This radiograph was taken as part of a foreign body
series in a patient with a bronchial foreign body. There
was no suspicion of cervical spine injury. Note that the
neck is flexed. This amplifies the C2/C3
pseudosubluxation. Neck flexion also increases the
width of the prevertebral soft tissues. In a properly
positioned radiograph, the prevertebral soft tissue
thickness should be about half the width of the vertebral
bodies (as demonstrated in the two previous
radiographs:
If this space is widened, it suggests the presence of
a retropharyngeal abscess in a febrile patient with upper
airway symptoms or soft tissue edema or bleeding from
an occult cervical spine fracture in a trauma patient. In
the [Neck-3] radiograph, the prevertebral soft tissues
are excessively wide, but not because of an abscess or
bleeding. This finding is purely due to positioning in this
case. In this case, taking the radiograph with the neck
extended will probably "cure" the patient of the
pseudosubluxation and the prevertebral soft tissue
widening.
References
Fassier F. C1-C4 Fractures and Dislocations. In:
Letts RM (ed). Management of Pediatric Fractures.
New York, Churchill Livingstone, 1994, pp. 807-831.
Ozonoff MB. The Spine. In: Ozonoff MB. Pediatric
Orthopedic Radiology. Philadelpha, W.B. Saunders
Company, 1992, pp. 1-7.
Woodward GA. Neck Trauma. In: Fleisher GR,
Ludwig S. Texbook of Pediatric Emergency Medicine,
third edition. Baltimore, Williams & Wilkins, 1993, pp.
1124-1142.
Swischuk LE. Anterior Displacement of C2 in
Children: Physiologic or Pathologic? A Helpful
Differentiating Line. Radiology 1977;122:759-763.
Chung SMK. The Neck. In: Handbook of Pediatric
Orthopedics. New York, Van Nostrand Reinhold, 1986,
pp. 43-52.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page