Respiratory Distress and Abdominal Distention
Radiology Cases in Pediatric Emergency Medicine
Volume 3, Case 11
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
A previously healthy 6-week old female is brought to
the E.D. 10 minutes after experiencing a sudden onset
of difficulty breathing.
Exam: VS T37 (tympanic), P160, R60. A blood
pressure is not recorded. Oxygen saturation 90% in
room air. She is tired, pale appearing, and in moderate
respiratory distress. Oxygen saturation improves to
99% on oxygen by mask. Her skin is mottled. Capillary
refill time is about 4 seconds. Eyes clear. Oral mucosa
moist. Neck supple. Heart tachycardic and regular.
There is a grade 3/6 systolic murmur. No gallops are
heard. Lungs clear with good aeration. Abdomen
distended and firm. Severe hepatomegaly is noted.
There is a 4 cm strawberry hemangioma over the right
flank region. Pulses are slightly weak.
A nasogastric tube is inserted. Blood work is drawn
and a chest/abdomen radiograph is obtained in the E.D.
View AP radiograph.
 The chest portion of the radiograph shows
cardiomegaly. Although the central pulmonary
vascularity may be slightly prominent, the lungs are
largely obscured by the cardiomegaly. The abdomen is
distended, and there is a paucity of bowel gas. There is
a suggestion of an abdominal mass.
She was not noted to have any signs or symptoms
of cardiac disease prior to this incident. A CT scan of
the abdomen is obtained.
View abdominal CT scan.
The chest portion of the radiograph shows
cardiomegaly. Although the central pulmonary
vascularity may be slightly prominent, the lungs are
largely obscured by the cardiomegaly. The abdomen is
distended, and there is a paucity of bowel gas. There is
a suggestion of an abdominal mass.
She was not noted to have any signs or symptoms
of cardiac disease prior to this incident. A CT scan of
the abdomen is obtained.
View abdominal CT scan.
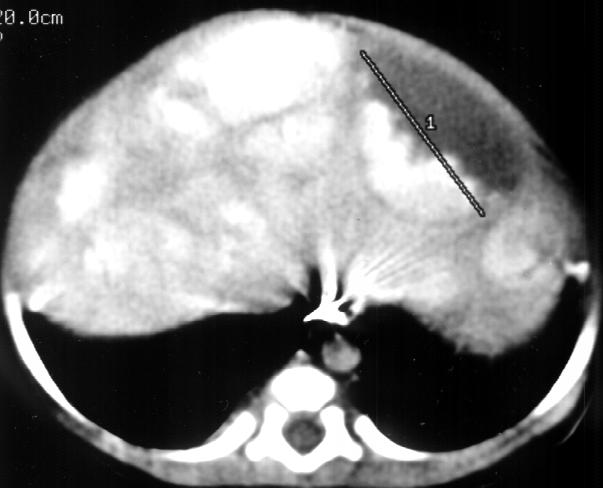 There are lobular vascular masses in the liver with
extreme hepatomegaly extending into the pelvis. These
are most likely hepatic cavernous hemangiomas. There
is a large cyst within the liver. It is unclear whether
there is significant hemorrhage into the cyst.
CBC WBC 7.9, 74% lymphs, 10% monos, 16% segs,
Hgb 8.6, Hct 25.3, platelets 234,000.
Questions:
1. Does this patient have congestive heart failure ?
2. Is this patient euvolemic or hypovolemic ?
3. Depending on your answer to the above, would
you administer volume expanding fluids and/or red
blood cells ?
The cardiomegaly noted on the chest radiograph is
quite prominent. However, it should be noted that
cardiomegaly does not always equate with cardiogenic
congestive heart failure, especially in this patient who
has no previous known history of cardiac disease.
Cardiomegaly seen on a chest radiograph could also be
due to pericardial fluid or high-output (non-cardiogenic)
congestive heart failure. The cardiac silhouette may
also appear to be enlarged if the lungs are hypoplastic
or if the film is taken during exhalation.
In our patient's case, the presence of a murmur
suggests the possibility of an anatomic cardiac lesion,
however, it could also be due to high-output failure.
The multiple vascular lesions in the liver are consistent
with high-output congestive heart failure due to
excessive arterio-venous shunting. The large
abdominal mass may be significantly compressing the
thoracic cavity so that the radiograph in essence is
similar to an expiratory view. This may give the heart
an enlarged appearance when, in fact, it is not
enlarged.
Based on the clinical information thus far, it is
difficult to determine with certainty the magnitude of
congestive heart failure, if any. An echocardiogram
would be useful in this situation.
A stat echocardiogram is performed. It shows slight
enlargement of the left atrium and left ventricle.
Contractility is normal. This study was able to rule out
cardiogenic causes of congestive heart failure. The
slight enlargement in the chamber sizes indicates that
some degree of congestive heart failure (CHF) is
present. It is probably high-output in nature due to
excessive arterio-venous shunting.
Now that we have determined that there is some
degree of high-output CHF, is this patient euvolemic or
hypovolemic and should we administer volume
expanding therapies (fluids and/or red blood cells) to
her? It is unclear what is responsible for her acute
deterioration. Her anemia may be due to hemolysis or
hemorrhage. However, it is unclear whether this has
worsened acutely, or whether this has occurred slowly.
Regardless, she is anemic and in failure. However, the
high-output CHF makes correcting her hemoglobin
more complication prone. Excessive volume expansion
in a patient with CHF of any type can result in acute
deterioration, despite correcting the anemia and/or
hypovolemia. Red blood cells are administered to her
cautiously. She is also treated simultaneously with
digoxin and furosemide.
She stabilized well and was transferred to the
intensive care unit. She continued to have difficulties in
maintaining her fluid balance despite intensive care
measures. She was transferred to a liver
transplantation center for selective embolization therapy
or transplantation.
There are lobular vascular masses in the liver with
extreme hepatomegaly extending into the pelvis. These
are most likely hepatic cavernous hemangiomas. There
is a large cyst within the liver. It is unclear whether
there is significant hemorrhage into the cyst.
CBC WBC 7.9, 74% lymphs, 10% monos, 16% segs,
Hgb 8.6, Hct 25.3, platelets 234,000.
Questions:
1. Does this patient have congestive heart failure ?
2. Is this patient euvolemic or hypovolemic ?
3. Depending on your answer to the above, would
you administer volume expanding fluids and/or red
blood cells ?
The cardiomegaly noted on the chest radiograph is
quite prominent. However, it should be noted that
cardiomegaly does not always equate with cardiogenic
congestive heart failure, especially in this patient who
has no previous known history of cardiac disease.
Cardiomegaly seen on a chest radiograph could also be
due to pericardial fluid or high-output (non-cardiogenic)
congestive heart failure. The cardiac silhouette may
also appear to be enlarged if the lungs are hypoplastic
or if the film is taken during exhalation.
In our patient's case, the presence of a murmur
suggests the possibility of an anatomic cardiac lesion,
however, it could also be due to high-output failure.
The multiple vascular lesions in the liver are consistent
with high-output congestive heart failure due to
excessive arterio-venous shunting. The large
abdominal mass may be significantly compressing the
thoracic cavity so that the radiograph in essence is
similar to an expiratory view. This may give the heart
an enlarged appearance when, in fact, it is not
enlarged.
Based on the clinical information thus far, it is
difficult to determine with certainty the magnitude of
congestive heart failure, if any. An echocardiogram
would be useful in this situation.
A stat echocardiogram is performed. It shows slight
enlargement of the left atrium and left ventricle.
Contractility is normal. This study was able to rule out
cardiogenic causes of congestive heart failure. The
slight enlargement in the chamber sizes indicates that
some degree of congestive heart failure (CHF) is
present. It is probably high-output in nature due to
excessive arterio-venous shunting.
Now that we have determined that there is some
degree of high-output CHF, is this patient euvolemic or
hypovolemic and should we administer volume
expanding therapies (fluids and/or red blood cells) to
her? It is unclear what is responsible for her acute
deterioration. Her anemia may be due to hemolysis or
hemorrhage. However, it is unclear whether this has
worsened acutely, or whether this has occurred slowly.
Regardless, she is anemic and in failure. However, the
high-output CHF makes correcting her hemoglobin
more complication prone. Excessive volume expansion
in a patient with CHF of any type can result in acute
deterioration, despite correcting the anemia and/or
hypovolemia. Red blood cells are administered to her
cautiously. She is also treated simultaneously with
digoxin and furosemide.
She stabilized well and was transferred to the
intensive care unit. She continued to have difficulties in
maintaining her fluid balance despite intensive care
measures. She was transferred to a liver
transplantation center for selective embolization therapy
or transplantation.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page