Test Your Skill In Distinguishing Obstruction From Ileus
Radiology Cases in Pediatric Emergency Medicine
Volume 3, Case 18
Corinne C. Chan-Nishina, MD
Patrice M.L. Tim-Sing, MD
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
Abdominal radiographs can be difficult to analyze. A
mechanical obstruction is often difficult to differentiate
from an adynamic ileus. The goal of this case
discussion is to help one to have a better understanding
of a mechanical obstruction versus an adynamic
(paralytic) ileus, and be able to make a distinction
between these two conditions. Sixteen abdominal
radiographs will be displayed to test your skill in
distinguishing a bowel obstruction from an ileus.
It is important to first look at those components that
are common to all films, such as the stomach, rectum,
and the hepatic and splenic flexures of the colon.
These areas are relatively fixed. Then, one should look
at the solid abdominal viscera, such as the liver, spleen,
kidneys, psoas muscles and bladder. Finally, an
examination of the lungs (lower portions), diaphragms,
bony structures and pelvis are important.
A mechanical obstruction is an impedance to the
passage of air or intestinal contents secondary to a
mechanical hindrance. Examples of this include
incarcerated inguinal hernia, bowel adhesions,
intussusception, volvulus, intestinal atresias,
intraluminal masses (tumors, bezoars, large stool
masses), and extrinsic bowel compression (Ladd's
bands, annular pancreas, etc.). In a paralytic
(adynamic) ileus, there is a temporary impedance to the
passage of air or contents secondary to uncoordinated
peristalsis or hypoperistalsis.
Adynamic ileus frequently occurs with major
abdominal, retroperitoneal and spinal surgery. It also
occurs frequently with inflammatory processes such as
sepsis, pneumonia, gastroenteritis, appendicitis,
peritonitis, pancreatitis and urinary tract infection. One
may have bowel disturbances and a resultant ileus with
hypokalemia, electrolyte disturbance, dehydration,
vasculitis, renal disease, neurogenic shock, sepsis,
drugs, hypothyroidism and idiopathic intestinal
pseudoobstruction. Although the most common cause
of an ileus is gastroenteritis, an ileus is not necessarily
a benign condition.
There are different criteria that one must look at
when trying to distinguish an ileus from an obstruction
on an abdominal radiograph. These include, the fixed
anatomy, gas distribution, degree of bowel distention,
air fluid levels, and arrangement of the bowel loops. It
should be noted that none of these criteria are
necessarily definitive in always distinguishing an ileus
from an obstruction.
Gas distribution:
A gasless abdomen is usually abnormal. Only rarely
is the abdomen truly gasless. However, radiographs
with an extreme paucity of gas (i.e., almost gasless)
should be treated with the same degree of suspicion as
a gasless abdominal radiograph. Although a gasless
abdomen is highly suggestive of a high obstruction, this
can also be seen with excessive vomiting, and/or
diarrhea. This picture can also occur in the early
stages of appendicitis, as well as in Addisonian crisis
(adrenal crisis). Occasionally, this occurs in patients
with marked cerebral depression such that their
swallowing is impaired.
In a mechanical obstruction, there is preferentially
more air proximal to the obstruction than distal to it.
Thus, in an obstruction, there is either too much gas in
the small bowel (and not much gas in the large bowel),
or too much gas in the large bowel (and not much gas
in the small bowel). In an adynamic ileus, there usually
is no preferential collection of air. There is too much air
or not much air in both the small and large bowel. This
pattern of distribution is not necessarily definitive.
When there is too much air in the small bowel, this may
be a small bowel obstruction which has been present
long enough to have allowed the colon gas to clear.
When there is too much air in the colon, this may be a
large bowel obstruction (e.g.., sigmoid volvulus) with a
competent ileocecal valve. If, however, there is too
much air in both parts of the bowel, you may have a
paralytic ileus, or a large bowel obstruction with an
incompetent ileocecal valve, or a small bowel
obstruction which is early or intermittent.
Another important point is that sometimes in a
mechanical obstruction, there is very little air present
and the intestinal loops are filled with fluid. In these
cases, the loops may appear as opaque sausage-like
structures in the abdomen or the bowel may be
isodense with the rest of the abdomen showing a
paucity of gas. On the upright view, the air may get
trapped in the valvulae conniventes (small bowel plicae
circulares [circular folds]) giving a "string of pearls" gas
pattern appearance.
Bowel dilatation:
Bowel dilatation is another important criteria that
needs to be considered. In a mechanical obstruction
one usually sees dilatation proximal to the site of
obstruction. In a bowel obstruction, the bowel dilatation
appearance in children is different from that generally
seen in adults. In infants and children, an obstruction
characteristically shows dilated bowel with SMOOTH
bowel walls. The degree of dilatation is not necessarily
excessive, but the smoothness of the bowel wall is
most notable. This smoothness is due to the loss of
plicae (circular folds) and haustration of the bowel due
to gaseous distention. In an obstruction where the
bowel is dilated, the bowel resembles "hoses" or
"sausages" where the bowel walls are smooth (the
normal bowel wall irregularity is lost).
Determining the level of the obstruction is often
difficult. It is often difficult to radiographically
distinguish small from large bowel in the infant. In older
children you may see cross striations which represent
the valvulae conniventes when the small bowel is
distended. These resemble the haustra of the large
bowel, however, they are more numerous and more
narrowly spaced. Haustra appear as indentations
which do not cross the lumen like these do, and the
indentations of haustra do not necessarily line up with
the opposite side. In paralytic ileus, the bowel loops all
dilate in proportion to each other. The colon usually
remains larger than the small intestine.
It is worth mentioning here that one can see short
segments of bowel dilatation adjacent to areas of
inflammation ("sentinel" loops). These are areas of
short segment paralytic ileus and when found in the
right upper quadrant, can represent cholecystitis,
pyelonephritis, hepatitis or traumatic disease. In the left
upper quadrant these are seen with pancreatitis,
pyelonephritis, or splenic injury. In the right lower
quadrant, it is seen with appendicitis, Meckel's
diverticulitis, or regional enteritis. These loops are rare
in the left lower quadrant, but can be seen with
salpingitis or cystitis in females.
Air-Fluid levels:
In mechanical obstruction, air-fluid levels can be
seen on the upright view. One can see short air-fluid
levels in both limbs of what look like hairpin loops of
intestine. The heights of the fluid levels are usually
different in any two limbs of one loop (resembles candy
canes). In a paralytic ileus, there may be few to
numerous sluggish air-fluid levels scattered throughout
the abdomen. An obstruction characteristically shows
many dilated air-fluid levels, while an ileus
characteristically shows fewer air-fluid levels that are
not dilated.
Arrangement of Bowel Loops:
One could also look at how orderly the intestinal
loops are arranged. In a mechanical obstruction the
dilated loops are often stacked one under the other in a
"step ladder" appearance (in a more orderly fashion) on
the SUPINE view (not the upright view). With an ileus,
the dilated loops tend to be less orderly, scattered
throughout the abdomen from top to bottom and side to
side. Perhaps another way at describing this
"orderliness", is that an obstruction resembles a bag of
sausages (a more orderly arrangement), while an ileus
resembles a bag of popcorn (a less orderly
arrangement). The sausages of a bowel obstruction
are due to dilated bowel while the popcorn of an ileus is
due to a generalized distribution of bowel gas and
better preservation of the bowel plicae and haustra.
In summary, one should evaluate abdominal films in a
stepwise fashion.
1. Look at the fixed anatomy. Do not forget the lungs.
2. Gas Distribution.
Obstruction: Too much air in the small bowel (and
not much gas in the large bowel) or too much air in the
large bowel (and not much gas in the small bowel).
Poor gas distribution or gasless.
Ileus: Good gas distribution over most of the
abdomen. Too much air in both large and small bowel.
Warning: This could also appear in large bowel
obstruction with an incompetent ileocecal valve, or in an
early or intermittent small bowel obstruction.
3. Bowel Dilatation.
Obstruction: Smooth bowel walls (resembles
sausages or a hose). Preferential dilatation of the
bowel proximal to the obstruction.
Ileus: Dilatation of the bowel in proportion to each
other, so that the colon remains larger than the small
intestine. Look for sentinel loops.
4. Air-fluid Levels.
Obstruction: Many dilated air-fluid levels in both
limbs of a given loop, at different heights (candy canes).
Ileus: Fewer and/or smaller (less dilated) air-fluid
levels scattered throughout the abdomen.
5. Arrangement of loops (supine view only).
Obstruction: Dilated loops arranged in "stepladder"
fashion. Orderly. A bag of sausages.
Ileus: Disorderly loops scattered throughout the
abdomen. A bag of popcorn.
Remember, presentations are variable, and not
always clear cut. Often, it is difficult to distinguish the
two, especially when there is a mixed paralytic and
mechanical obstruction. A high index of suspicion
should remain when the clinical and radiographic
information is unclear. Conditions such as
intussusception, volvulus, and appendicitis are surgical
emergencies that require a timely diagnosis and
intervention. These conditions may not have definitive
findings on plain radiographs. Other diagnostic studies
or surgical intervention may be necessary if these
conditions are still suspected after the completion of
plain film radiographs.
Now test your skill in distinguishing obstruction from
ileus in this series of 16 pediatric abdominal
radiographs. All of these patients are vomiting with
varying degrees of abdominal pain. No histories are
given here except for the patient's age and sex. In
reality, the radiographic findings should be interpreted in
conjunction with the patient's clinical findings. Two
views are shown in each case. The view on the left is a
supine view. The view on the right is an upright view
unless otherwise specified.
Case A: 18-month old male.
View Case A.
 Interpretation of Case A
Gas Distribution: There are pockets of gas
scattered in several areas of the abdomen. There is
gas in the small bowel, colon, and rectum.
Bowel Dilatation: No excessively dilated bowel. The
bowel walls are not smooth. Haustra and plicae are
preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Large loops are not present.
Impression: Within normal limits.
Case B: 7-day old female.
View Case B.
Interpretation of Case A
Gas Distribution: There are pockets of gas
scattered in several areas of the abdomen. There is
gas in the small bowel, colon, and rectum.
Bowel Dilatation: No excessively dilated bowel. The
bowel walls are not smooth. Haustra and plicae are
preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Large loops are not present.
Impression: Within normal limits.
Case B: 7-day old female.
View Case B.
 Interpretation of Case B
Gas Distribution: There are pockets of gas
scattered in several areas of the abdomen. There is
gas in the small bowel, colon, and rectum.
Bowel Dilatation: There is mild dilation of the bowel,
mostly in the colon. The dilated segment of bowel in
the left upper quadrant shows relatively smooth bowel
walls. However, most of the bowel does not show this.
In other words, the haustra and plicae of most of the
bowel are well preserved.
Air-Fluid Levels: None.
Arrangement of Loops: The loops are not arranged
in an orderly pattern.
Impression: Ileus.
Case C: 17-day old male.
View Case C.
Interpretation of Case B
Gas Distribution: There are pockets of gas
scattered in several areas of the abdomen. There is
gas in the small bowel, colon, and rectum.
Bowel Dilatation: There is mild dilation of the bowel,
mostly in the colon. The dilated segment of bowel in
the left upper quadrant shows relatively smooth bowel
walls. However, most of the bowel does not show this.
In other words, the haustra and plicae of most of the
bowel are well preserved.
Air-Fluid Levels: None.
Arrangement of Loops: The loops are not arranged
in an orderly pattern.
Impression: Ileus.
Case C: 17-day old male.
View Case C.
 Interpretation of Case C
Gas Distribution: There is gas over most of the
abdomen. There are loops of bowel mostly in the
central abdomen. The dilated loops are mostly small
bowel.
Bowel Dilatation: The bowel walls are smooth
indicating that the bowel is dilated.
Air-Fluid Levels: There are multiple short air fluid
levels on the upright film (hair pin loops).
Arrangement of Loops: Orderly, although not truly in
a stepladder fashion. The arrangement here resembles
a bag of sausages more so that a bag of popcorn.
Impression: Small bowel obstruction. In this age,
the mostly likely cause is an incarcerated inguinal
hernia. This is confirmed clinically.
Case D: 1-month old female.
View Case D.
Interpretation of Case C
Gas Distribution: There is gas over most of the
abdomen. There are loops of bowel mostly in the
central abdomen. The dilated loops are mostly small
bowel.
Bowel Dilatation: The bowel walls are smooth
indicating that the bowel is dilated.
Air-Fluid Levels: There are multiple short air fluid
levels on the upright film (hair pin loops).
Arrangement of Loops: Orderly, although not truly in
a stepladder fashion. The arrangement here resembles
a bag of sausages more so that a bag of popcorn.
Impression: Small bowel obstruction. In this age,
the mostly likely cause is an incarcerated inguinal
hernia. This is confirmed clinically.
Case D: 1-month old female.
View Case D.
 Interpretation of Case D
Gas Distribution: There is a lot of gas in the small
and large bowel distributed throughout the abdomen.
Bowel Dilatation: The degree of bowel dilation here
is proportional throughout. In other words, the large
bowel is slightly dilated, as is the small bowel.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement of
dilated bowel. This resembles a bag of popcorn rather
than a bag of sausages.
Impression: Ileus. The differential is extensive,
including gastroenteritis, urinary tract infection, etc.
However, an ileus is still compatible with several
surgical conditions such as appendicitis.
Case E: 3-1/2 year old male.
View Case E.
Interpretation of Case D
Gas Distribution: There is a lot of gas in the small
and large bowel distributed throughout the abdomen.
Bowel Dilatation: The degree of bowel dilation here
is proportional throughout. In other words, the large
bowel is slightly dilated, as is the small bowel.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement of
dilated bowel. This resembles a bag of popcorn rather
than a bag of sausages.
Impression: Ileus. The differential is extensive,
including gastroenteritis, urinary tract infection, etc.
However, an ileus is still compatible with several
surgical conditions such as appendicitis.
Case E: 3-1/2 year old male.
View Case E.
 Interpretation of Case E
Gas Distribution: Increased gaseous distribution in
both small and large bowel, with more colonic
involvement. Gas is also present in the rectum.
Bowel Dilatation: Note the smooth bowel walls
resulting in the "sausage-like" appearance of some of
the loops. There are several areas of extreme dilation.
The stomach is also very dilated.
Air-Fluid Levels: Multiple loops of bowel with air
fluid levels. The typical "candy cane" appearance is not
very dramatic.
Arrangement of Loops: The loops are stacked in a
somewhat orderly fashion. However, this is not definite.
The "arrangement" should be best determined on the
supine flat view and not the upright view. Although this
arrangement resembles a bag of sausages more so
than a bag of popcorn, this is not as clear-cut as in
other cases.
Impression: The gas distribution throughout the
bowel suggests that this is not an obstruction.
However, the reason for the extreme bowel dilatation is
uncertain. This is still suspicious for an obstruction.
Note the frothy density over the left flank area (supine
view). This probably represents fecal matter. Though a
fecal obstruction is possible, a BE or an UGI series
would be helpful to evaluate other causes of obstruction
such as malrotation or Hirshsprung's disease. A
contrast enema and an UGI series were performed on
this patient. Both were normal. His symptoms and
bowel dilation gradually resolved after several enemas
and bowel movements.
Case F: 7-month old male.
View Case F.
Interpretation of Case E
Gas Distribution: Increased gaseous distribution in
both small and large bowel, with more colonic
involvement. Gas is also present in the rectum.
Bowel Dilatation: Note the smooth bowel walls
resulting in the "sausage-like" appearance of some of
the loops. There are several areas of extreme dilation.
The stomach is also very dilated.
Air-Fluid Levels: Multiple loops of bowel with air
fluid levels. The typical "candy cane" appearance is not
very dramatic.
Arrangement of Loops: The loops are stacked in a
somewhat orderly fashion. However, this is not definite.
The "arrangement" should be best determined on the
supine flat view and not the upright view. Although this
arrangement resembles a bag of sausages more so
than a bag of popcorn, this is not as clear-cut as in
other cases.
Impression: The gas distribution throughout the
bowel suggests that this is not an obstruction.
However, the reason for the extreme bowel dilatation is
uncertain. This is still suspicious for an obstruction.
Note the frothy density over the left flank area (supine
view). This probably represents fecal matter. Though a
fecal obstruction is possible, a BE or an UGI series
would be helpful to evaluate other causes of obstruction
such as malrotation or Hirshsprung's disease. A
contrast enema and an UGI series were performed on
this patient. Both were normal. His symptoms and
bowel dilation gradually resolved after several enemas
and bowel movements.
Case F: 7-month old male.
View Case F.
 Interpretation of Case F
Gas Distribution: Relatively gasless in both large
and small bowel. This is a poor gas distribution.
Bowel Dilatation: In some of the few bowel loops
that are seen, the bowel walls appear smooth.
Air-Fluid Levels: There are no obvious air-fluid
levels. However, in the upright view, the central
abdomen shows the presence of two bowel loops
resembling arches that are air-fluid levels which do not
have the typical candy cane appearance. The candy
cane appearance of air-fluid levels is usually not seen in
infants.
Arrangement of Loops: It is difficult to comment on
the arrangement given the minimal gas pattern.
Impression: Probable obstruction based mainly on
the paucity of gas and its distribution. Since these
radiographs are highly suspicious, the next
recommended exam should be an ultrasound and/or a
BE to evaluate the possibility of intussusception or
appendicitis. An intussusception is often the cause of a
bowel obstruction associated with a paucity of gas on
plain radiographs A BE performed in this patient
demonstrated an intussusception.
Case G: Newborn male.
View Case G.
Interpretation of Case F
Gas Distribution: Relatively gasless in both large
and small bowel. This is a poor gas distribution.
Bowel Dilatation: In some of the few bowel loops
that are seen, the bowel walls appear smooth.
Air-Fluid Levels: There are no obvious air-fluid
levels. However, in the upright view, the central
abdomen shows the presence of two bowel loops
resembling arches that are air-fluid levels which do not
have the typical candy cane appearance. The candy
cane appearance of air-fluid levels is usually not seen in
infants.
Arrangement of Loops: It is difficult to comment on
the arrangement given the minimal gas pattern.
Impression: Probable obstruction based mainly on
the paucity of gas and its distribution. Since these
radiographs are highly suspicious, the next
recommended exam should be an ultrasound and/or a
BE to evaluate the possibility of intussusception or
appendicitis. An intussusception is often the cause of a
bowel obstruction associated with a paucity of gas on
plain radiographs A BE performed in this patient
demonstrated an intussusception.
Case G: Newborn male.
View Case G.
 Interpretation of Case G
In this case, only a supine view is shown on the left.
The image on the right is a contrast enema study.
Gas Distribution: There is poor gas distribution with
only 3 dilated loops of bowel, triple bubbles, probably
representing high (i.e., proximal) small bowel loops.
There is some gas in the left lower quadrant. This
cannot be the colon since there is no gas in any other
intervening bowel segments evident.
Bowel Dilatation: As noted above, dilation is present
in the loops seen. There is no colon gas evident.
Air-Fluid Levels: An upright or lateral decubitus view
is not shown here.
Arrangement of Loops: Too few to comment.
Impression: This is a proximal small bowel
obstruction. The contrast enema on the right shows a
microcolon indicating the absence of bowel contents
passing to the colon during gestation. In a proximal
small bowel obstruction, a microcolon is usually not
present. The presence of a microcolon suggests that
the distal small bowel is also atretic. This patient was
ultimately diagnosed with a long segment small bowel
atresia. Note that the contrast enema study also shows
the cecum in the wrong position. It should be in the
right lower quadrant, but it appears to be more medial
than its expected positions. Malpositioning of the
cecum is highly indicative of a malrotation.
Case H: 3-day old female.
View Case H.
Interpretation of Case G
In this case, only a supine view is shown on the left.
The image on the right is a contrast enema study.
Gas Distribution: There is poor gas distribution with
only 3 dilated loops of bowel, triple bubbles, probably
representing high (i.e., proximal) small bowel loops.
There is some gas in the left lower quadrant. This
cannot be the colon since there is no gas in any other
intervening bowel segments evident.
Bowel Dilatation: As noted above, dilation is present
in the loops seen. There is no colon gas evident.
Air-Fluid Levels: An upright or lateral decubitus view
is not shown here.
Arrangement of Loops: Too few to comment.
Impression: This is a proximal small bowel
obstruction. The contrast enema on the right shows a
microcolon indicating the absence of bowel contents
passing to the colon during gestation. In a proximal
small bowel obstruction, a microcolon is usually not
present. The presence of a microcolon suggests that
the distal small bowel is also atretic. This patient was
ultimately diagnosed with a long segment small bowel
atresia. Note that the contrast enema study also shows
the cecum in the wrong position. It should be in the
right lower quadrant, but it appears to be more medial
than its expected positions. Malpositioning of the
cecum is highly indicative of a malrotation.
Case H: 3-day old female.
View Case H.
 Interpretation of Case H
Gas Distribution: Generalized presence of gas
throughout all quadrants.
Bowel Dilatation: The degree of bowel dilatation is
proportional. The right lower quadrant may
demonstrate some smooth bowel walls, but this is
probably just the descending colon. Some of the
haustra in these segments are still preserved. For the
remainder of the bowel, the haustra and plicae are well
preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement
resembling a bag of popcorn.
Impression: Ileus.
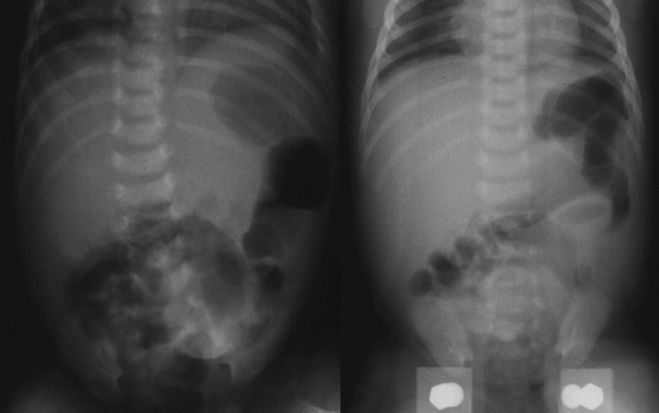
Case I: 2-1/2 year old female.
View Case I.
Interpretation of Case H
Gas Distribution: Generalized presence of gas
throughout all quadrants.
Bowel Dilatation: The degree of bowel dilatation is
proportional. The right lower quadrant may
demonstrate some smooth bowel walls, but this is
probably just the descending colon. Some of the
haustra in these segments are still preserved. For the
remainder of the bowel, the haustra and plicae are well
preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement
resembling a bag of popcorn.
Impression: Ileus.
Case I: 2-1/2 year old female.
View Case I.
 Interpretation of Case I
Gas Distribution: Well distributed throughout all
quadrants.
Bowel Dilatation: There are two dilated regions
seen on the supine view in both lower quadrants.
However, the bowel walls do not appear smooth. The
typical sausage or hose appearance of dilated small
bowel is not present. The haustra and plicae are still
fairly well preserved.
Air-Fluid Levels: The upright view shows many
small air fluid levels. The typical hairpin or candy cane
appearance is not present indicating that these air
fluid levels are small and not present in large loops.
Arrangement of Loops: Disorderly loops resembling
a bag of popcorn more so than a bag of sausages
(supine view).
Impression: Moderate ileus versus partial
obstruction. An ileus is more likely.
Case J: 3-year old female.
View Case J.
Interpretation of Case I
Gas Distribution: Well distributed throughout all
quadrants.
Bowel Dilatation: There are two dilated regions
seen on the supine view in both lower quadrants.
However, the bowel walls do not appear smooth. The
typical sausage or hose appearance of dilated small
bowel is not present. The haustra and plicae are still
fairly well preserved.
Air-Fluid Levels: The upright view shows many
small air fluid levels. The typical hairpin or candy cane
appearance is not present indicating that these air
fluid levels are small and not present in large loops.
Arrangement of Loops: Disorderly loops resembling
a bag of popcorn more so than a bag of sausages
(supine view).
Impression: Moderate ileus versus partial
obstruction. An ileus is more likely.
Case J: 3-year old female.
View Case J.
 Interpretation of Case J
Gas Distribution: There is gas distributed
throughout the abdomen. Most of the gas present is in
the colon.
Bowel Dilatation: There is moderate dilation of the
colonic regions. There is a dilated loop of small bowel
on the left (supine view) which overlaps the colon. The
haustra and plicae are preserved. No sausages or
hoses are seen (i.e., no smooth bowel walls are
present).
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement
resembling a bag of popcorn more so than a bag of
sausages.
Impression: Ileus.
Case K: 9-day old male.
View Case K.
Interpretation of Case J
Gas Distribution: There is gas distributed
throughout the abdomen. Most of the gas present is in
the colon.
Bowel Dilatation: There is moderate dilation of the
colonic regions. There is a dilated loop of small bowel
on the left (supine view) which overlaps the colon. The
haustra and plicae are preserved. No sausages or
hoses are seen (i.e., no smooth bowel walls are
present).
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly arrangement
resembling a bag of popcorn more so than a bag of
sausages.
Impression: Ileus.
Case K: 9-day old male.
View Case K.
 Interpretation of Case K
Gas Distribution: Poor distribution. Although gas is
present throughout most of the abdomen, its distribution
appears to be limited to just a few bowel segments.
Bowel Dilatation: Marked bowel distention though
difficult to determine small versus large bowel. The
bowel walls are smooth.
Air-Fluid Levels: Multiple air-fluid levels mostly on
the left. Hair pins and candy canes are not present.
Arrangement of Loops: Not very helpful in this case.
The arrangement is best evaluated on the supine view
which is not obviously orderly or disorderly. In other
words, it is not easy to say whether this arrangement
resembles a bag of sausages or a bag of popcorn.
Impression: Obstruction based mainly on the gas
distribution and the degree of bowel dilatation. This is
not a normal abdominal series for a 9-day old. A
contrast enema demonstrated a transition zone
consistent with Hirschsprung's disease.
Case L: 12-month old female.
View Case L.
Interpretation of Case K
Gas Distribution: Poor distribution. Although gas is
present throughout most of the abdomen, its distribution
appears to be limited to just a few bowel segments.
Bowel Dilatation: Marked bowel distention though
difficult to determine small versus large bowel. The
bowel walls are smooth.
Air-Fluid Levels: Multiple air-fluid levels mostly on
the left. Hair pins and candy canes are not present.
Arrangement of Loops: Not very helpful in this case.
The arrangement is best evaluated on the supine view
which is not obviously orderly or disorderly. In other
words, it is not easy to say whether this arrangement
resembles a bag of sausages or a bag of popcorn.
Impression: Obstruction based mainly on the gas
distribution and the degree of bowel dilatation. This is
not a normal abdominal series for a 9-day old. A
contrast enema demonstrated a transition zone
consistent with Hirschsprung's disease.
Case L: 12-month old female.
View Case L.
 Interpretation of Case L
Gas Distribution: Small areas of gas are present
throughout the entire abdomen. Many of the areas are
foamy suggesting the presence of excessive amounts
of stool.
Bowel Dilatation: Most of the bowel is not dilated.
There is a modest paucity of gas. There are two dilated
loops in the RLQ on the supine view (RLQ sentinel
loops).
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly. Despite the
paucity of gas, the supine view resembles a bag of
popcorn more so than a bag of sausages.
Impression: Ileus. RLQ sentinel loops raise the
possibility of appendicitis.
Case M: 7-month old female.
View Case M.
Interpretation of Case L
Gas Distribution: Small areas of gas are present
throughout the entire abdomen. Many of the areas are
foamy suggesting the presence of excessive amounts
of stool.
Bowel Dilatation: Most of the bowel is not dilated.
There is a modest paucity of gas. There are two dilated
loops in the RLQ on the supine view (RLQ sentinel
loops).
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly. Despite the
paucity of gas, the supine view resembles a bag of
popcorn more so than a bag of sausages.
Impression: Ileus. RLQ sentinel loops raise the
possibility of appendicitis.
Case M: 7-month old female.
View Case M.
 Interpretation of Case M
Gas Distribution: There is a definite paucity of gas
which is poorly distributed.
Bowel Dilatation: Nothing obvious.
Air-Fluid Levels: None.
Arrangement of Loops: Not a useful sign here
because of the paucity of gas.
Other comments: There is a "target sign" in the
right upper quadrant. The target sign is discussed in
detail in Case 2 of Volume 1. The target is faintly
visible as a doughnut shape (with the doughnut center
still present) in the right upper quadrant below the liver
(supine view). This is subtle. You may have to turn
down the room lights and adjust the contrast and
brightness on your monitor. This sign indicates the
presence of an intussusception. This radiograph also
demonstrates the "absent liver edge" sign (liver edge
not well defined in any view), which is also a sign of
intussusception (though less specific than the target
sign). If you have difficulty identifying the target and
liver edge findings in this radiograph, review Case 2 of
Volume 1 for other examples that are easier to identify.
Impression: Suggestive of an obstruction based
mainly on the paucity of gas. The target sign indicates
the presence of an intussusception. A barium enema
confirmed an intussusception.
Case N: 22-month old.
View Case N.
Interpretation of Case M
Gas Distribution: There is a definite paucity of gas
which is poorly distributed.
Bowel Dilatation: Nothing obvious.
Air-Fluid Levels: None.
Arrangement of Loops: Not a useful sign here
because of the paucity of gas.
Other comments: There is a "target sign" in the
right upper quadrant. The target sign is discussed in
detail in Case 2 of Volume 1. The target is faintly
visible as a doughnut shape (with the doughnut center
still present) in the right upper quadrant below the liver
(supine view). This is subtle. You may have to turn
down the room lights and adjust the contrast and
brightness on your monitor. This sign indicates the
presence of an intussusception. This radiograph also
demonstrates the "absent liver edge" sign (liver edge
not well defined in any view), which is also a sign of
intussusception (though less specific than the target
sign). If you have difficulty identifying the target and
liver edge findings in this radiograph, review Case 2 of
Volume 1 for other examples that are easier to identify.
Impression: Suggestive of an obstruction based
mainly on the paucity of gas. The target sign indicates
the presence of an intussusception. A barium enema
confirmed an intussusception.
Case N: 22-month old.
View Case N.
 Interpretation of Case N
Gas Distribution: Good distribution except for one
portion in the LUQ. Although the upright view appears
to be somewhat gasless with most of the gas seen
localized to the upper abdomen only, the supine view
shows a better distribution of gas.
Bowel Dilatation: There are no dilated regions. The
haustra and plicae are well preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly.
Other Comments: The supine view demonstrates
"thumb printing" suggesting bowel wall edema such as
that seen in colitis. This is best seen in the LUQ
region (or left middle region) where the colon shows
thumb-shaped indentations into its lumen.
Impression: Ileus, colitis.
Case O: 11-month old male.
View Case O.
Interpretation of Case N
Gas Distribution: Good distribution except for one
portion in the LUQ. Although the upright view appears
to be somewhat gasless with most of the gas seen
localized to the upper abdomen only, the supine view
shows a better distribution of gas.
Bowel Dilatation: There are no dilated regions. The
haustra and plicae are well preserved.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly.
Other Comments: The supine view demonstrates
"thumb printing" suggesting bowel wall edema such as
that seen in colitis. This is best seen in the LUQ
region (or left middle region) where the colon shows
thumb-shaped indentations into its lumen.
Impression: Ileus, colitis.
Case O: 11-month old male.
View Case O.
 Interpretation of Case O
Gas Distribution: Poorly distributed. Gas is
concentrated in the left upper quadrants in both the
supine and upright views.
Bowel Dilatation: There are two dilated bowel
segments seen on the supine view. The bowel walls
are smooth and resemble sausages.
Air-Fluid Levels: None.
Arrangement of Loops: Orderly. Note the two
dilated bowel segments on the supine view are stacked
on top of each other resembling a step ladder. Also,
this view clearly resembles a bag of sausages (only two
big ones), rather than a bag of popcorn.
Impression: Obstruction. A barium enema in this
case demonstrated intussusception.
Case P: 6-1/2 year old male.
View Case P.
Interpretation of Case O
Gas Distribution: Poorly distributed. Gas is
concentrated in the left upper quadrants in both the
supine and upright views.
Bowel Dilatation: There are two dilated bowel
segments seen on the supine view. The bowel walls
are smooth and resemble sausages.
Air-Fluid Levels: None.
Arrangement of Loops: Orderly. Note the two
dilated bowel segments on the supine view are stacked
on top of each other resembling a step ladder. Also,
this view clearly resembles a bag of sausages (only two
big ones), rather than a bag of popcorn.
Impression: Obstruction. A barium enema in this
case demonstrated intussusception.
Case P: 6-1/2 year old male.
View Case P.
 Interpretation of Case P
Gas Distribution: Well distributed except for a
paucity of gas in the left lower quadrant.
Bowel Dilatation: The haustra and plicae are well
preserved. No smooth bowel walls are visible. The
caliber of the bowel is proportional to the normal bowel
size.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly. Does not
resemble a bag of sausages. Nor does it truly
resemble a bag of popcorn. However, there is no order
to the arrangement.
Impression: Ileus. There is a possible appendicolith
in the right lower quadrant (spherical density). This is
highly suggestive of acute appendicitis. This again
stresses the point, that an ileus is not necessarily
benign.
References
1. Swischuk LE. The Abdomen. In: Swischuk LE.
Emergency Radiology of the Acutely Ill or Injured Child,
second edition. Baltimore, Williams & Wilkins, 1986,
pp. 153-164.
2. Swischuk LE. The Alimentary Tract. In:
Radiology of the Newborn and Young Infant, second
edition. Baltimore, Williams & Wilkins, 1980, pp.
487-490.
3. Kirks DR. The Gastrointestinal Tract. In:
Practical Pediatric and Diagnostic Radiology of Infants
and Children. Boston, Little, Brown and Company,
1984, pp. 551-553.
4. Parker BR. The Abdomen and Gastrointestinal
Tract. In: Silverman FN, Kuhn JP. Caffey's Pediatric
X-Ray Diagnosis, Ninth edition. St. Louis, Mosby,
1993, pp. 1059-1089.
5. Squire LF, Novelline RA. The Abdominal Plain
Film: Distended Stomach, Small Bowel, Colon, Free
Fluid and Free Air. In: Fundamentals of Radiology, 4th
edition. Cambridge, MA, Harvard University Press,
1988, pp. 194-205.
Interpretation of Case P
Gas Distribution: Well distributed except for a
paucity of gas in the left lower quadrant.
Bowel Dilatation: The haustra and plicae are well
preserved. No smooth bowel walls are visible. The
caliber of the bowel is proportional to the normal bowel
size.
Air-Fluid Levels: None.
Arrangement of Loops: Disorderly. Does not
resemble a bag of sausages. Nor does it truly
resemble a bag of popcorn. However, there is no order
to the arrangement.
Impression: Ileus. There is a possible appendicolith
in the right lower quadrant (spherical density). This is
highly suggestive of acute appendicitis. This again
stresses the point, that an ileus is not necessarily
benign.
References
1. Swischuk LE. The Abdomen. In: Swischuk LE.
Emergency Radiology of the Acutely Ill or Injured Child,
second edition. Baltimore, Williams & Wilkins, 1986,
pp. 153-164.
2. Swischuk LE. The Alimentary Tract. In:
Radiology of the Newborn and Young Infant, second
edition. Baltimore, Williams & Wilkins, 1980, pp.
487-490.
3. Kirks DR. The Gastrointestinal Tract. In:
Practical Pediatric and Diagnostic Radiology of Infants
and Children. Boston, Little, Brown and Company,
1984, pp. 551-553.
4. Parker BR. The Abdomen and Gastrointestinal
Tract. In: Silverman FN, Kuhn JP. Caffey's Pediatric
X-Ray Diagnosis, Ninth edition. St. Louis, Mosby,
1993, pp. 1059-1089.
5. Squire LF, Novelline RA. The Abdominal Plain
Film: Distended Stomach, Small Bowel, Colon, Free
Fluid and Free Air. In: Fundamentals of Radiology, 4th
edition. Cambridge, MA, Harvard University Press,
1988, pp. 194-205.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page