Right-Sided Abdominal Pain in a 10-Year Old
Radiology Cases in Pediatric Emergency Medicine
Volume 5, Case 18
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
This is a 10-year old with an acute onset of sharp
constant epigastric pain without radiation. The pain is
worse when lying down and when ambulating. He is
unable to jump. He has had three loose stools without
blood, mucus, or foul odor. He has some nausea, but
no vomiting, dysuria, fever, or cold symptoms.
Exam: VS T36.7 (TM), P80, R18, BP 134/84,
oxygen saturation 100% in room air. He is in moderate
distress due to pain. He does not appear to be toxic.
Eyes normal. Ears normal. There is bilateral maxillary
sinus tenderness. Pharynx red with enlarged tonsils
(no exudates). Neck supple without adenopathy. Heart
regular without murmurs. Lungs clear. Abdomen flat,
guarding, moderate non-localized tenderness and
rebound. A Murphy's sign cannot be reliably elicited.
Bowel sounds are active. No masses. No hernias.
Testes are normal. No CVA tenderness. Extremities
with good pulses and perfusion. Strength good.
An abdominal series and laboratory studies are
ordered. He is given a dose of oral antacids.
View abdominal series [Supine view]
 [Upright view]
[Upright view]
 Laboratory studies: CBC WBC 7,000 with 24%
lymphs, 5% monos, and 71% segs. Hgb 13, Hct 34,
platelet count 329,000. Amylase 66. UA normal.
The abdominal series shows some dilated bowel.
The gas pattern is not distributed well. Most of the gas
is in the central abdomen. The flat view shows a small
opacification in the right upper quadrant. There may be
other small densities overlying the bowel gas inferiorly,
but this is not certain. The upright view shows a small
opacification on the right but it is located lower than the
opacity seen on the supine film. Either this is a different
lesion, or the opacification is mobile, and it moves
inferiorly with gravity.
Since this is not likely to be a vascular calcification in
a 10-year old, the differential includes urolithiasis,
cholelithiasis, or a high appendicolith.
View a close-up of the calcifications.
Laboratory studies: CBC WBC 7,000 with 24%
lymphs, 5% monos, and 71% segs. Hgb 13, Hct 34,
platelet count 329,000. Amylase 66. UA normal.
The abdominal series shows some dilated bowel.
The gas pattern is not distributed well. Most of the gas
is in the central abdomen. The flat view shows a small
opacification in the right upper quadrant. There may be
other small densities overlying the bowel gas inferiorly,
but this is not certain. The upright view shows a small
opacification on the right but it is located lower than the
opacity seen on the supine film. Either this is a different
lesion, or the opacification is mobile, and it moves
inferiorly with gravity.
Since this is not likely to be a vascular calcification in
a 10-year old, the differential includes urolithiasis,
cholelithiasis, or a high appendicolith.
View a close-up of the calcifications.
 Following the antacid and a period of observation,
his abdominal pain subsides without other analgesics.
He does not have CVA tenderness and there is no
hematuria making urolithiasis unlikely. His exam is now
only positive for mild right upper quadrant tenderness
without rebound. His bowel sounds are active. He can
ambulate well and he tells the staff that he wants to go
home. He is given discharge instructions regarding
abdominal pain. He is instructed to see his physician in
the morning.
In a follow-up visit with his physician, he has
continued to improve. However, as a follow-up to
identify the cause of the right upper quadrant
opacifications, an abdominal ultrasound is performed.
View ultrasound.
Following the antacid and a period of observation,
his abdominal pain subsides without other analgesics.
He does not have CVA tenderness and there is no
hematuria making urolithiasis unlikely. His exam is now
only positive for mild right upper quadrant tenderness
without rebound. His bowel sounds are active. He can
ambulate well and he tells the staff that he wants to go
home. He is given discharge instructions regarding
abdominal pain. He is instructed to see his physician in
the morning.
In a follow-up visit with his physician, he has
continued to improve. However, as a follow-up to
identify the cause of the right upper quadrant
opacifications, an abdominal ultrasound is performed.
View ultrasound.
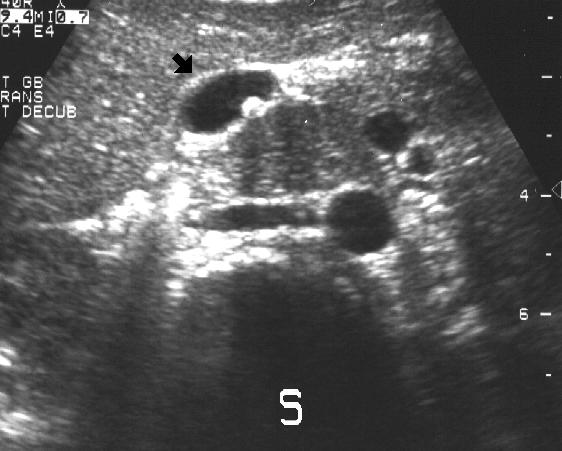 This ultrasound transducer is over the anterior
abdomen in the right upper quadrant. The liver is
shown here. The "S" is the spine. The black arrow
points to the gall bladder. A stone is seen in the gall
bladder in this view. Note the echo "shadow" cast by
the stone. Other views reveal other stones in the gall
bladder. There are no stones in the common duct.
Discussion
Gallstones in children are not felt to be common.
However, many of them are asymptomatic. While most
gallstones in children are classically associated with
hemolytic disease and hemoglobinopathies (hereditary
spherocytosis, sickle cell anemia, thalassemia, etc.), an
increasing incidence of cholesterol stones have been
noted. It is now felt that cholesterol stones are more
common than pigment stones in children. Cholecystitis
and cholelithiasis are more common in childhood than is
generally appreciated. Other children at increased risk
include premature infants on furosemide and children
receiving parenteral nutrition.
The usual clinical presentation of cholecystitis and
cholelithiasis is often not present in children. Most
children present with non-specific abdominal pain. Liver
function studies may be normal. Plain film abdominal
radiographs may reveal calcifications, however, they
are often normal. Ultrasound is the easiest means of
making a definitive diagnosis of cholelithiasis. Acute
cholecystitis may require a bile duct flow study such as
a nuclear medicine excretion study. Cholecystitis may
sometimes occur without cholelithiasis (acalculous
cholecystitis).
Pediatric experience with newer therapeutic
approaches such as lithotripsy and bile acid stone
dissolution are lacking. Treatment has been
traditionally surgical, however, this may be evolving.
References
Holcomb GW. Gallbladder Disease. In: Welch KJ,
Randolph JG, Ravitch MM, etal (eds). Pediatric
Surgery, fourth edition. Year Book Medical Publishers,
Inc., Chicago, 1986, pp. 1060-1067.
Karrer FM, Lilly JR, Hall RJ. Biliary Tract Disorders
and Portal Hypertension. In: Ashcraft
KW, Holder TM. Pediatric Surgery, second edition.
W.B. Saunders Company, Philadelphia, 1993, pp.
493-494.
Swischuk LE. The Abdomen. In: Swischuk LE.
Emergency Imaging of the Acutely Ill or Injured Child,
third edition. Williams & Wilkins, Baltimore, 1994, pp.
254-258.
This ultrasound transducer is over the anterior
abdomen in the right upper quadrant. The liver is
shown here. The "S" is the spine. The black arrow
points to the gall bladder. A stone is seen in the gall
bladder in this view. Note the echo "shadow" cast by
the stone. Other views reveal other stones in the gall
bladder. There are no stones in the common duct.
Discussion
Gallstones in children are not felt to be common.
However, many of them are asymptomatic. While most
gallstones in children are classically associated with
hemolytic disease and hemoglobinopathies (hereditary
spherocytosis, sickle cell anemia, thalassemia, etc.), an
increasing incidence of cholesterol stones have been
noted. It is now felt that cholesterol stones are more
common than pigment stones in children. Cholecystitis
and cholelithiasis are more common in childhood than is
generally appreciated. Other children at increased risk
include premature infants on furosemide and children
receiving parenteral nutrition.
The usual clinical presentation of cholecystitis and
cholelithiasis is often not present in children. Most
children present with non-specific abdominal pain. Liver
function studies may be normal. Plain film abdominal
radiographs may reveal calcifications, however, they
are often normal. Ultrasound is the easiest means of
making a definitive diagnosis of cholelithiasis. Acute
cholecystitis may require a bile duct flow study such as
a nuclear medicine excretion study. Cholecystitis may
sometimes occur without cholelithiasis (acalculous
cholecystitis).
Pediatric experience with newer therapeutic
approaches such as lithotripsy and bile acid stone
dissolution are lacking. Treatment has been
traditionally surgical, however, this may be evolving.
References
Holcomb GW. Gallbladder Disease. In: Welch KJ,
Randolph JG, Ravitch MM, etal (eds). Pediatric
Surgery, fourth edition. Year Book Medical Publishers,
Inc., Chicago, 1986, pp. 1060-1067.
Karrer FM, Lilly JR, Hall RJ. Biliary Tract Disorders
and Portal Hypertension. In: Ashcraft
KW, Holder TM. Pediatric Surgery, second edition.
W.B. Saunders Company, Philadelphia, 1993, pp.
493-494.
Swischuk LE. The Abdomen. In: Swischuk LE.
Emergency Imaging of the Acutely Ill or Injured Child,
third edition. Williams & Wilkins, Baltimore, 1994, pp.
254-258.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page