Radiology Cases In Neonatology
Copyright 1996, Loren Yamamoto
Performance Improvement Project
Loren Yamamoto, MD, MPH
Department of Pediatrics and Quality Management Department,
Kapiolani Medical Center For Women And Children
Department of Pediatrics,
University of Hawaii John A. Burns School of Medicine
Identify significant abnormalities in each of the following neonatal radiographs. Answers are displayed below the radiographs.
These x-ray files load slowly. Please be patient . . .
Requires 256 color driver and JPEG capability. Some radiographs may not display well without optimal color drivers.
Case 1:
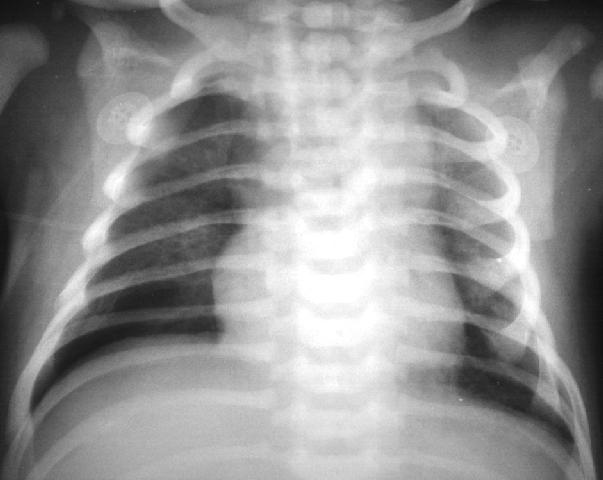
Subtle right pneumothorax.
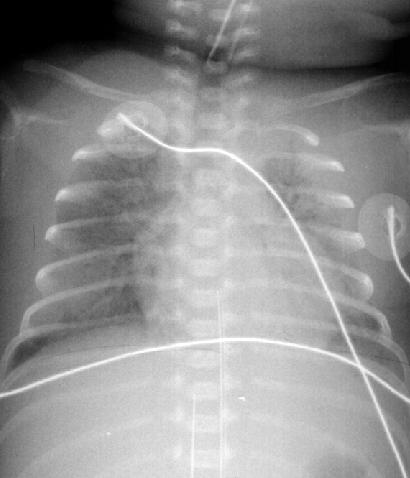
Case 2:

Respiratory distress syndrome. ETT is too high. You must always note the ETT position and reposition it if necessary.
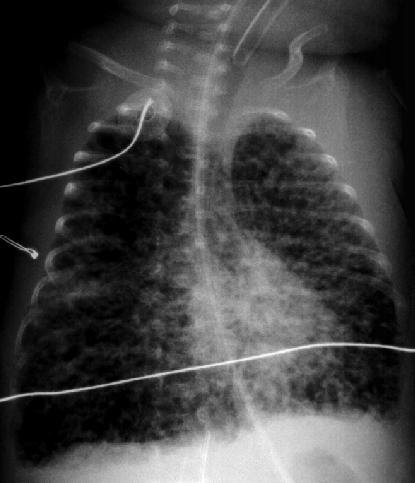
Case 3:

UAC at T11. UVC above diaphragm. How can you distinguish UAC from UVC. You really need to see the umbilicus portion of this radiograph to follow the lines up. Without this information, one can't be certain, but most likely, the line on the patient's left more closely follows the path of the aorta so this is probably the UAC. The line on the patient's right more closely follows the hepatic vein so this is probably the UVC.
Case 4:

Left diaphragmatic hernia. There is also a small right pneumothorax, but this is difficult to see since bowel gas overlies it.
Case 5:

UAC at L2 (too high). Note how the UAC dips down and then up as it enters the umbilical cord into the aorta. This is the hallmark of a UAC and not a UVC.
Case 6:

ETT too low. It should be repositioned.
Case 7:

Pneumatosis intestinalis. Note the air visible in the bowel wall. The air dissects the bowel wall giving it a double lined appearance (ie., railroad tracks without the ties). Necrotizing enterocolitis.
Case 8:

ETT too low. Reposition it. UAC OK at T9.
Case 9:

RDS. ETT in satisfactory position, but note that there are two tubes up there. The smaller one is an NG tube that is in the upper esophagus (too high). The UAC is OK at T4. There is some radiocontrast in the lower bowel.
Case 10:

Right pneumothorax. Pulmonary interstitial emphysema. UAC OK at T7.
Case 11:

In this case the UVC is on the patient's left and the UAC is on the patient's right. I'm not sure why this is. However, there is significant rotation in the positioning of the radiograph. Note that the UVC goes straight up, while the UAC goes down and then up as it enters the body through the umbilicus.
Case 12:

ETT in right mainstem. Too low. Reposition it.
Case 13:

Pneumomediastinum. Note how the thymus is elevated (pushed up by mediastinal air), most visible on the right. There is also a small right pneumothorax.
Case 14:

UVC looping in heart (up IVC and into RA). UAC at T2 (up aorta on left with the tip in the aortic arch). UVC and UAC are too high.
Case 15:

Right pneumothorax.
Case 16:

Pneumatosis intestinalis. Note the double linear density of the bowel wall indicative of air within the bowel wall (intramural air). There are also subtle air densities over the liver. This suggests that there is air in the portal circulation (intraportal air). Both findings indicate necrotizing enterocolitis.
Case 17:

Pulmonary interstitial emphysema. ETT too high. UAC just above diaphragm.
Case 18:

Right diaphragmatic hernia and left pneumothorax.
Case 19:
Respiratory distress syndrome. ETT too high. UVC in liver on right.
Case 20:

Pneumatosis intestinalis. Very obvious case. Tremendous amount of air in bowel walls.
Case 21:

Which line is the UAC and which is the UVC? High line follows aorta so this is the UAC. The low line follows the liver so it is the UVC. Can't see the bottom of this x-ray to be more definitive than this.
Case 22:
Name three things wrong with this x-ray? 1) Severe pulmonary interstitial emphysema. 2) ETT too high. 3) UAC too low.
Case 23:

ETT too low. Left pneumothorax.
Return to Univ. Hawaii Dept. Pediatrics Home Page
Web Page Author:
Loren Yamamoto, MD, MPH
Professor of Pediatrics
University of Hawaii John A. Burns School of Medicine
loreny@hawaii.edu