Elbow Ossification Centers in a Child
Radiology Cases in Pediatric Emergency Medicine
Volume 1, Case 11
Alson S. Inaba, MD
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
A 7 year old male presents to the ED with isolated
right elbow pain three hours after falling on his
out-stretched right arm while roller blading. The patient
did not sustain any other trauma to his head, neck or
trunk. He has not complained of any numbness or
tingling in his right hand post-injury.
Exam: The right upper extremity from the clavicle to
the tip of the fingers is atraumatic in appearance
without any obvious angulation or swelling. The patient
exhibits full range of motion about the shoulder and
wrist. There is no tenderness over the anatomic
"snuffbox" region. The elbow has no obvious swelling,
and the elbow circumference (of the affected arm) is
equal to the elbow circumference of the non-affected
arm. There is very mild, diffuse tenderness about the
right elbow (without any specific point tenderness). He
has no pain with active elbow flexion, extension,
supination, or pronation. Although you clinically do not
suspect any fracture of the right elbow region, the
patient's mother is very anxious and demands an x-ray
of her son's elbow. Radiographs of the right elbow are
obtained.
View elbow radiographs.
 Questions:
1) How many ossification centers are present in this
radiograph and what are the names of these
ossification centers?
2) Are the ossification centers in their correct
(expected) anatomic positions?
3) Are there any fractures present in this
radiograph, and if so where?
Discussion & Teaching Points:
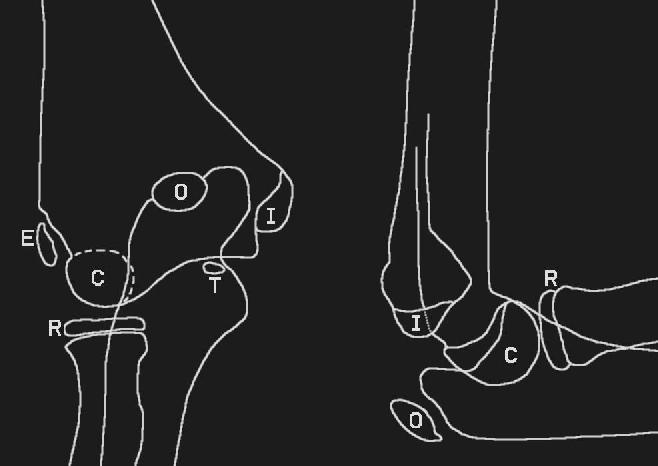
1) There are 6 ossification centers around the elbow
joint. These ossification centers all appear at different
ages and they all fuse to the adjacent bones at various
ages. It is not clinically important to memorize the
specific ages of when these ossification centers appear
or fuse. However, it is clinically important to realize that
the ossification centers always appear in a specific
sequence. The mnemonic of the order of appearance
of the individual ossification centers is C-R-I-T-O-E:
Capitellum, Radial head, Internal (medial) epicondyle,
Trochlea, Olecranon, External (lateral) epicondyle.
Remember that the anatomic position of the body
places the upper extremities in external rotation
(supination at the elbows) such that the antecubital
fossa faces anteriorly. Thus, the external epicondyle is
on the radial side of the elbow, while the internal
epicondyle is on the ulnar side of the elbow.
The ages at which these ossification centers appear
are highly variable, but as a general guide, remember
1-3-5-7-9-11 years. Note that our patient in this case is
7 years old but all six ossification centers are present.
This illustrates that this age sequence is just a guide
since the age ranges are highly variable.
Review elbow diagram.
Questions:
1) How many ossification centers are present in this
radiograph and what are the names of these
ossification centers?
2) Are the ossification centers in their correct
(expected) anatomic positions?
3) Are there any fractures present in this
radiograph, and if so where?
Discussion & Teaching Points:
1) There are 6 ossification centers around the elbow
joint. These ossification centers all appear at different
ages and they all fuse to the adjacent bones at various
ages. It is not clinically important to memorize the
specific ages of when these ossification centers appear
or fuse. However, it is clinically important to realize that
the ossification centers always appear in a specific
sequence. The mnemonic of the order of appearance
of the individual ossification centers is C-R-I-T-O-E:
Capitellum, Radial head, Internal (medial) epicondyle,
Trochlea, Olecranon, External (lateral) epicondyle.
Remember that the anatomic position of the body
places the upper extremities in external rotation
(supination at the elbows) such that the antecubital
fossa faces anteriorly. Thus, the external epicondyle is
on the radial side of the elbow, while the internal
epicondyle is on the ulnar side of the elbow.
The ages at which these ossification centers appear
are highly variable, but as a general guide, remember
1-3-5-7-9-11 years. Note that our patient in this case is
7 years old but all six ossification centers are present.
This illustrates that this age sequence is just a guide
since the age ranges are highly variable.
Review elbow diagram.
 2) Knowing the C-R-I-T-O-E mnemonic is helpful in
determining whether a small piece of bone about the
elbow joint represents an avulsion fragment or an
ossification center. The ossification centers always
appear in the order specified in the mnemonic
C-R-I-T-O-E.
3) Example: If you see only three accessory bony
fragments about an elbow joint, these bony pieces
should be in the areas of the capitellum, radial head
and the internal (medial) epicondyle. If one of the three
bony fragments is in the area where you would expect
to see the external epicondyle, then that piece actually
represents an avulsion fracture of the distal, lateral
humerus, rather than a normal external epicondyle.
4) Whenever evaluating an injured extremity, the
most important aspect of the examination is to assess
the neurovascular integrity of the affected extremity.
5) Always remember to palpate the entire extremity
(including the clavicles) in all children who present after
falling on the out-stretched arm.
6) Always remember to document whether or not
the patient who has fallen on the out-stretched hand
has any tenderness over the anatomic "snuffbox"
(scaphoid bone). Any patient with tenderness over the
scaphoid (navicular) bone must be treated (splinted with
orthopedic referral) as an occult scaphoid fracture
until proven otherwise (even if the initial scaphoid
views do not reveal any evidence of a fracture). Refer
to Case 14 (A Hand Contusion) for more details.
Radiographic Findings: No evidence of
elbow effusion. Normal anterior humeral line
and a normal radiocapitellar line. (Refer to Case
12, Radiographic Examination of the Elbow, to learn
how to assess elbow effusions and how to measure the
anterior humeral and radiocapitellar lines). All six
ossification centers are present in their expected
anatomic positions.
Overall radiographic interpretation: Normal right
elbow with normal ossification centers.
2) Knowing the C-R-I-T-O-E mnemonic is helpful in
determining whether a small piece of bone about the
elbow joint represents an avulsion fragment or an
ossification center. The ossification centers always
appear in the order specified in the mnemonic
C-R-I-T-O-E.
3) Example: If you see only three accessory bony
fragments about an elbow joint, these bony pieces
should be in the areas of the capitellum, radial head
and the internal (medial) epicondyle. If one of the three
bony fragments is in the area where you would expect
to see the external epicondyle, then that piece actually
represents an avulsion fracture of the distal, lateral
humerus, rather than a normal external epicondyle.
4) Whenever evaluating an injured extremity, the
most important aspect of the examination is to assess
the neurovascular integrity of the affected extremity.
5) Always remember to palpate the entire extremity
(including the clavicles) in all children who present after
falling on the out-stretched arm.
6) Always remember to document whether or not
the patient who has fallen on the out-stretched hand
has any tenderness over the anatomic "snuffbox"
(scaphoid bone). Any patient with tenderness over the
scaphoid (navicular) bone must be treated (splinted with
orthopedic referral) as an occult scaphoid fracture
until proven otherwise (even if the initial scaphoid
views do not reveal any evidence of a fracture). Refer
to Case 14 (A Hand Contusion) for more details.
Radiographic Findings: No evidence of
elbow effusion. Normal anterior humeral line
and a normal radiocapitellar line. (Refer to Case
12, Radiographic Examination of the Elbow, to learn
how to assess elbow effusions and how to measure the
anterior humeral and radiocapitellar lines). All six
ossification centers are present in their expected
anatomic positions.
Overall radiographic interpretation: Normal right
elbow with normal ossification centers.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page