A Second Look at a Coin in the Stomach
Radiology Cases in Pediatric Emergency Medicine
Volume 2, Case 9
Loren G. Yamamoto, MD, MPH
Alson S. Inaba, MD
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
This is a 20 month old female who presents to the
emergency department after swallowing a coin,
according to two older children who were playing with
her at the time. They don't know what type of coin it
was. Her mother has not noted any difficulty
swallowing, drooling, or respiratory difficulty.
Exam VS T37.1 (tympanic), P100, R36, BP 100/65,
oxygen saturation 99% in room air. Alert, active, no
distress, no drooling. Eyes clear, TM's normal. Oral
clear, moist mucosa. Neck supple. Heart regular
without murmurs. Lungs clear. No stridor, no
wheezing, no coughing, no tachypnea, no retractions.
Abdomen soft, flat, non-tender, bowel sounds active.
Color, perfusion good. Speech normal for age.
Ambulating well.
An AP radiograph of her trunk is taken.
View AP film.
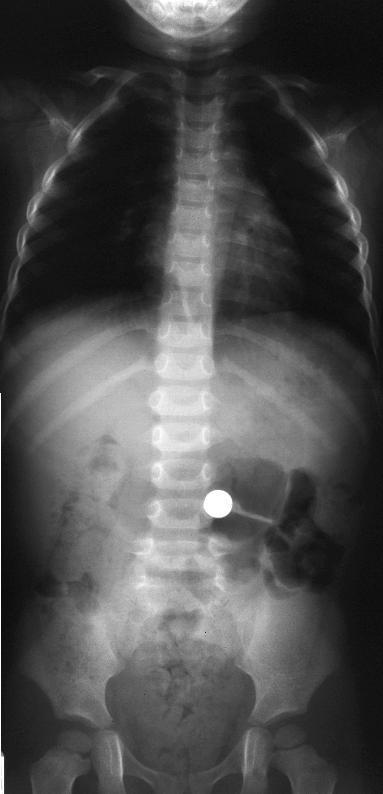 This radiograph shows a coin in her stomach.
However, upon closer inspection, it has an unusual
appearance.
View close-up of coin.
This radiograph shows a coin in her stomach.
However, upon closer inspection, it has an unusual
appearance.
View close-up of coin.
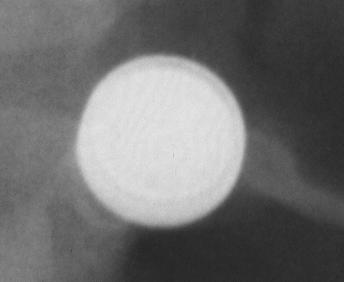 The "coin" shows an internal ring just inside its
perimeter. This internal ring indicates that this is a disc
battery, not a coin. Since disk batteries (also called
button batteries) have different GI consequences
compared to coins, it is important to distinguish an
ingested coin from a disc battery by history or
radiographically. Disc batteries will often have the
characteristic internal ring appearance if taken in the AP
direction. If taken in the lateral position (on edge), it
may show a bulge on one side (bilaminar appearance).
When viewed obliquely, it may be difficult to distinguish
a coin from a disc battery since none of these signs
may be radiographically evident.
View lineup of disc batteries.
The "coin" shows an internal ring just inside its
perimeter. This internal ring indicates that this is a disc
battery, not a coin. Since disk batteries (also called
button batteries) have different GI consequences
compared to coins, it is important to distinguish an
ingested coin from a disc battery by history or
radiographically. Disc batteries will often have the
characteristic internal ring appearance if taken in the AP
direction. If taken in the lateral position (on edge), it
may show a bulge on one side (bilaminar appearance).
When viewed obliquely, it may be difficult to distinguish
a coin from a disc battery since none of these signs
may be radiographically evident.
View lineup of disc batteries.
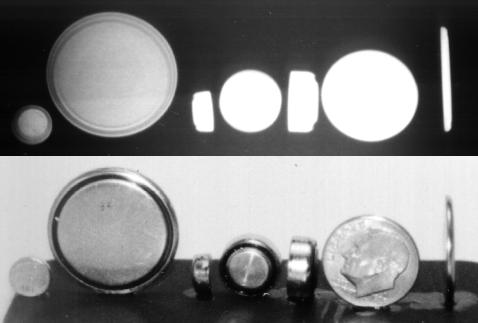 This lineup shows a radiograph of a series of 6 disc
batteries and a dime. The first disc battery on the left
has the positive terminal facing toward us. The second
battery from the left has its negative terminal facing
toward us. On this second battery, the black plastic
insulator is visible in the photograph. However, the
radiograph of both the first and the second disc
batteries show the internal ring sign of the plastic
insulator. The black plastic insulator on the first battery
is on the other side of the battery. The radiograph will
still show the internal ring of the plastic insulator
regardless of which way the battery is facing (AP or
PA). The fourth battery from the left also shows a
plastic insulator, but the radiograph of this battery does
not show the internal ring. It could be absent because
the battery casing is thicker than the first and second
batteries. Thus, the absence of the internal ring
radiographically does not rule out a disc battery since
the appearance of the internal ring is highly dependent
on the degree of X-ray penetration, the angle of the
battery, and the thickness of the battery casing.
The third and fifth batteries from the left are viewed
from the side. On its side view, the battery has a
rectangular appearance with a bulge on one end. This
bulge represents the negative terminal of the battery as
shown in the corresponding photo below it. The
radiographic shadow also identifies this bulge which can
be described as frosting on the cake (bilaminar
appearance). However, this radiographic sign may be
absent if the battery is oriented obliquely, or if the
battery is very thin. The battery to the extreme right is
oriented on edge. The side view of this battery does
not easily show the bulge of the negative terminal
because this battery is very thin as can be seen in the
photograph.
Disc batteries contain various chemicals depending
on the type. Standard dry cell batteries contain
zinc-carbon, alkaline, and nickel-cadmium compounds,
but these are generally not found in disc batteries. Disc
batteries generally contain silver oxide, mercuric oxide,
or lithium salts. They may also contain concentrated
caustics of potassium or sodium hydroxide. Most disc
batteries in use today are the silver oxide or lithium
types. However, many inexpensive or disposable child
toys may still contain the less expensive mercuric oxide
disc batteries.
Disc batteries lodged in the esophagus can
potentially cause serious problems in three ways: 1)
Direct pressure necrosis (similar to coins or other inert
foreign bodies). 2) Caustic injury due to the leakage of
sodium or potassium hydroxide from a leaking battery.
3) The esophagus can also sustain injury from low
voltage burns from a disc battery that still has a charge.
For these reasons, all disc batteries lodged in the
esophagus should be removed expeditiously to avoid
these injuries.
Disc batteries that leak can also cause toxicity from
the absorption of metal compounds. Mercuric oxide
batteries can potentially cause mercury poisoning
resulting in gastritis, vomiting, and hypovolemic shock.
This is not likely to occur for several reasons: 1) Most
disc batteries do not leak. They negotiate the GI tract
and are passed intact in the stool. 2) Most of the
mercuric oxide from old batteries is converted to
insoluble metallic mercury which is not absorbed. 3)
Any mercuric oxide that happens to leak out of the
battery is converted to elemental mercury in the
presence of gastric acids.
Silver salts from silver oxide batteries may be
corrosive, but they are minimally toxic. Lithium is a
highly reactive metal under extreme conditions such as
fire. Complications have not been reported in the
literature following ingestion of a lithium disc battery.
Most disc batteries will pass through the GI tract
without difficulty. A radiograph should be taken to
localize the battery. Esophageal batteries should be
removed expeditiously. If the battery is beyond the
esophagus, the patient may be sent home and
instructed to watch for symptoms of toxicity and
passage of the battery in the stool by straining all
stools. Induction of emesis is generally not successful
and it may be potentially harmful since the battery is
potentially caustic. A repeat radiograph is usually not
indicated until 4 to 7 days after the ingestion if the
battery has not been recovered. Cathartics may
accelerate passage of the battery. If passage is
delayed, the risk of leakage and the potential for
complications depending on the contents of the battery
must be assessed to determine the need for
endoscopic or surgical removal. Although most
batteries will remain intact for two weeks or more, some
batteries may have defective casings or they may be
old and be leaking at the time the battery is swallowed.
References.
Poisindex. Volume 83, Expires 2/28/95. Micromdex
Inc.
Kuhns DW, Dire DJ. Button battery ingestions. Ann
Emerg Med 1989;18:293.
Maves MD, Lloyd TV, Carithers JS. Radiographic
identification of ingested disk batteries. Pediatr Radiol
1986;16:154.
Sheikh A. Button battery ingestions in children.
Pediatr Emerg Care 1993;9:224.
Temple DM, McNeese MC. Hazards of battery
ingestion. Pediatrics 1983;71:100.
This lineup shows a radiograph of a series of 6 disc
batteries and a dime. The first disc battery on the left
has the positive terminal facing toward us. The second
battery from the left has its negative terminal facing
toward us. On this second battery, the black plastic
insulator is visible in the photograph. However, the
radiograph of both the first and the second disc
batteries show the internal ring sign of the plastic
insulator. The black plastic insulator on the first battery
is on the other side of the battery. The radiograph will
still show the internal ring of the plastic insulator
regardless of which way the battery is facing (AP or
PA). The fourth battery from the left also shows a
plastic insulator, but the radiograph of this battery does
not show the internal ring. It could be absent because
the battery casing is thicker than the first and second
batteries. Thus, the absence of the internal ring
radiographically does not rule out a disc battery since
the appearance of the internal ring is highly dependent
on the degree of X-ray penetration, the angle of the
battery, and the thickness of the battery casing.
The third and fifth batteries from the left are viewed
from the side. On its side view, the battery has a
rectangular appearance with a bulge on one end. This
bulge represents the negative terminal of the battery as
shown in the corresponding photo below it. The
radiographic shadow also identifies this bulge which can
be described as frosting on the cake (bilaminar
appearance). However, this radiographic sign may be
absent if the battery is oriented obliquely, or if the
battery is very thin. The battery to the extreme right is
oriented on edge. The side view of this battery does
not easily show the bulge of the negative terminal
because this battery is very thin as can be seen in the
photograph.
Disc batteries contain various chemicals depending
on the type. Standard dry cell batteries contain
zinc-carbon, alkaline, and nickel-cadmium compounds,
but these are generally not found in disc batteries. Disc
batteries generally contain silver oxide, mercuric oxide,
or lithium salts. They may also contain concentrated
caustics of potassium or sodium hydroxide. Most disc
batteries in use today are the silver oxide or lithium
types. However, many inexpensive or disposable child
toys may still contain the less expensive mercuric oxide
disc batteries.
Disc batteries lodged in the esophagus can
potentially cause serious problems in three ways: 1)
Direct pressure necrosis (similar to coins or other inert
foreign bodies). 2) Caustic injury due to the leakage of
sodium or potassium hydroxide from a leaking battery.
3) The esophagus can also sustain injury from low
voltage burns from a disc battery that still has a charge.
For these reasons, all disc batteries lodged in the
esophagus should be removed expeditiously to avoid
these injuries.
Disc batteries that leak can also cause toxicity from
the absorption of metal compounds. Mercuric oxide
batteries can potentially cause mercury poisoning
resulting in gastritis, vomiting, and hypovolemic shock.
This is not likely to occur for several reasons: 1) Most
disc batteries do not leak. They negotiate the GI tract
and are passed intact in the stool. 2) Most of the
mercuric oxide from old batteries is converted to
insoluble metallic mercury which is not absorbed. 3)
Any mercuric oxide that happens to leak out of the
battery is converted to elemental mercury in the
presence of gastric acids.
Silver salts from silver oxide batteries may be
corrosive, but they are minimally toxic. Lithium is a
highly reactive metal under extreme conditions such as
fire. Complications have not been reported in the
literature following ingestion of a lithium disc battery.
Most disc batteries will pass through the GI tract
without difficulty. A radiograph should be taken to
localize the battery. Esophageal batteries should be
removed expeditiously. If the battery is beyond the
esophagus, the patient may be sent home and
instructed to watch for symptoms of toxicity and
passage of the battery in the stool by straining all
stools. Induction of emesis is generally not successful
and it may be potentially harmful since the battery is
potentially caustic. A repeat radiograph is usually not
indicated until 4 to 7 days after the ingestion if the
battery has not been recovered. Cathartics may
accelerate passage of the battery. If passage is
delayed, the risk of leakage and the potential for
complications depending on the contents of the battery
must be assessed to determine the need for
endoscopic or surgical removal. Although most
batteries will remain intact for two weeks or more, some
batteries may have defective casings or they may be
old and be leaking at the time the battery is swallowed.
References.
Poisindex. Volume 83, Expires 2/28/95. Micromdex
Inc.
Kuhns DW, Dire DJ. Button battery ingestions. Ann
Emerg Med 1989;18:293.
Maves MD, Lloyd TV, Carithers JS. Radiographic
identification of ingested disk batteries. Pediatr Radiol
1986;16:154.
Sheikh A. Button battery ingestions in children.
Pediatr Emerg Care 1993;9:224.
Temple DM, McNeese MC. Hazards of battery
ingestion. Pediatrics 1983;71:100.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page