Test Your Skill In Reading Pediatric Elbows
Radiology Cases in Pediatric Emergency Medicine
Volume 2, Case 18
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
Pediatric elbow radiographs can be difficult to
interpret unless one adheres to a methodical means of
looking for specific abnormalities. Unlike other long
bones, bony injuries of the elbow are not obvious.
However, by following a few simple rules, the
identification of these injuries need not be difficult.
In Volume 1 of this text disk, several cases were
reviewed to illustrate some of the methods to
radiographically diagnose fractures in the elbow region.
You may want to review these cases before proceeding
with the interpretation of the current series of elbow
radiographs.
Volume 1, Case 11: Elbow Ossification Centers in a
Child. This case discusses the sequence that elbow
ossification centers appear. CRITOE is the mnemonic
used to remember this sequence: Capitellum, radial
head, internal epicondyle, trochlea, olecranon, and
external epicondyle.
Volume 1, Case 12: Radiographic Examination of
the Elbow - The Hourglass Sign. This case discusses
the appearance of fat pads, supracondylar fractures,
and the importance of obtaining a true lateral film.
Volume 1, Case 15: Monteggia's Injury. This case
discusses the association of an ulna fracture with a
radial head dislocation. The radial head should point
directly at the capitellum in all views.
Volume 1, Case 17: Elbow Sprain in a Child. This
case describes the difficulty in appreciating radial head
fractures.
Volume 1, Case 19: Swollen Elbow with a Normal
X-ray. This case describes some fractures that are
difficult to see on conventional views of the elbow.
When a fracture injury is clinically obvious, but the
radiographs fail to reveal a fracture, one should still be
highly suspicious of an occult fracture.
Summary of Elbow Radiographic Examination:
A. Examine the lateral view first.
1. Examine the anterior fat pad. The presence of
an anterior fat pad is normal. It should be small and
appear to be flat against the anterior surface of the
humerus. If it is large or it appears to be triangular in
shape as if its lower tip is being displaced upwards, this
indicates the presence of an elbow joint effusion. Joint
effusions are highly correlated with visible fractures and
occult fractures.
2. Look for the presence of a posterior fat pad. A
lucency posterior to the humerus at the olecranon fossa
(a posterior fat pad) is always an abnormal sign and
indicates the presence of an elbow joint effusion.
3. Examine the anterior humeral line. Draw a line
down the anterior border of the humerus. This line
should bisect the capitellum. If this line fails to bisect
the capitellum, this indicates the presence of a fracture
in the supracondylar region displacing the capitellum
(usually posteriorly) or a Salter-Harris Type I fracture
between the capitellum and the distal humerus.
4. Examine the radial head. The shape of the radial
head should show a smooth metaphysis. Any angles in
the metaphysis may indicate a radial head fracture.
5. Examine the radiocapitellar line. The radius
should point directly at the capitellum in all views. If the
radius does not point directly at the capitellum, this
indicates a dislocation of the radial head.
6. In conjunction with the AP view, count the
number of ossification centers seen in the radiographs
and determine their location to see if any of them are
appearing out of the CRITOE sequence.
7. Examine the olecranon and the remainder of the
ulna for irregularities in the cortex. An ossification
center over the olecranon may resemble a fracture.
The presence or absence of tenderness over the
olecranon may help to establish a diagnosis.
8. Check for the Hourglass sign. Look for an
hourglass or Figure-of-8 shape at the distal humerus.
The absence of this indicates that the radiograph is
not a true lateral view of the elbow. An oblique view of
the elbow may obscure some of the radiographic
findings described above.
B. Examine the AP view.
1. Look carefully at the distal humerus for any
lucencies indicating a supracondylar fracture. This
region is highly fracture prone in children. Fractures in
this area may be subtle. Examine the metaphysis for
any interruption or angles. Lateral condyle fractures are
usually small, but result in significant swelling clinically.
2. Examine the shape of the radial head as noted
in item 4 above.
3. Examine the radiocapitellar line as noted in item
5 above.
Clinical Correlation.
Since radial head fractures are often difficult to
appreciate radiographically, clinical findings can often
be helpful in suspecting an occult fracture that is not
radiographically obvious. Tenderness over the radial
head or pain with supination and pronation should raise
the suspicion of a radial head fracture in children
without a history indicating a nursemaid's elbow. A
swollen elbow is almost always indicative of a fracture.
If a nursemaids's elbow has been ruled out and the
child is still not using the arm, this is highly suspicious
for an occult fracture, though not necessarily in the
elbow.
Summary Outline:
1. Anterior fat pad.
2. Posterior fat pad.
3. Anterior humeral line.
4. Radial head contour.
5. Radiocapitellar line.
6. Ossification centers. CRITOE
7. Hourglass sign.
8. Distal humerus.
9. Ulna/Olecranon.
10. Clinical correlation.
Now try your skill on the case examples. Use the
summary outline above to develop a methodical means
to examine the radiographs.
View Case A.
 Interpretation of Case A
1. Anterior fat pad: Very faint, if visible at all.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Slightly abnormal.
4. Radial head contour: Probably normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present.
8. Distal humerus: Abnormal. There is a lucency
through the distal lateral humerus indicative of a lateral
condyle fracture.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Lateral Condyle
fracture. Potential Salter-Harris Type II.
View Case B.
Interpretation of Case A
1. Anterior fat pad: Very faint, if visible at all.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Slightly abnormal.
4. Radial head contour: Probably normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present.
8. Distal humerus: Abnormal. There is a lucency
through the distal lateral humerus indicative of a lateral
condyle fracture.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Lateral Condyle
fracture. Potential Salter-Harris Type II.
View Case B.
 Interpretation of Case B
1. Anterior fat pad: Abnormally large and displaced
upward and anteriorly. Diagnostic of a joint effusion.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Abnormal. The capitellum
is clearly posterior to the anterior humeral line. This
indicates that there is a supracondylar fracture
displacing the distal segment posteriorly or a
Salter-Harris type I fracture between the capitellum and
humerus displacing the capitellum posteriorly.
4. Radial head contour: Normal.
5. Radiocapitellar line: Almost normal. The radial
head points at the general direction of the capitellum.
However, a line drawn down the long axis of the radius
does not precisely intersect the center of the capitellum.
This is probably due to the displacement of the
capitellum as noted in item 3 above, rather than a radial
head dislocation.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present. However, note that the
hourglass is crinkled because of the supracondylar
fracture.
8. Distal humerus: Abnormal. The metaphysis of
the distal humerus on the AP view shows two
irregularities. On the right, the smooth contour of the
distal metaphysis is interrupted by an angle in the
cortex. On the left, the smooth contour of the distal
metaphysis is interrupted by a bulge in the cortex. Both
irregularities indicate a supracondylar fracture. Within
the body of the distal humerus, it is difficult to
appreciate any fracture lines.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture.
View Case C.
Interpretation of Case B
1. Anterior fat pad: Abnormally large and displaced
upward and anteriorly. Diagnostic of a joint effusion.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Abnormal. The capitellum
is clearly posterior to the anterior humeral line. This
indicates that there is a supracondylar fracture
displacing the distal segment posteriorly or a
Salter-Harris type I fracture between the capitellum and
humerus displacing the capitellum posteriorly.
4. Radial head contour: Normal.
5. Radiocapitellar line: Almost normal. The radial
head points at the general direction of the capitellum.
However, a line drawn down the long axis of the radius
does not precisely intersect the center of the capitellum.
This is probably due to the displacement of the
capitellum as noted in item 3 above, rather than a radial
head dislocation.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present. However, note that the
hourglass is crinkled because of the supracondylar
fracture.
8. Distal humerus: Abnormal. The metaphysis of
the distal humerus on the AP view shows two
irregularities. On the right, the smooth contour of the
distal metaphysis is interrupted by an angle in the
cortex. On the left, the smooth contour of the distal
metaphysis is interrupted by a bulge in the cortex. Both
irregularities indicate a supracondylar fracture. Within
the body of the distal humerus, it is difficult to
appreciate any fracture lines.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture.
View Case C.
 Interpretation of Case C
1. Anterior fat pad: Not abnormally enlarged. It is
fairly small and it lies flat against the anterior humerus.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Abnormal. The capitellum
is clearly posterior to the anterior humeral line. This
indicates that there is a supracondylar fracture
displacing the distal segment posteriorly or a
Salter-Harris type I fracture between the capitellum and
humerus displacing the capitellum posteriorly.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present. However, again note
that the hourglass is crinkled.
8. Distal humerus: Abnormal. The metaphysis of
the distal lateral (on the right) humerus on the AP view
shows a large buckling irregularity of the cortex. On the
medial side (left), the smooth contour of the distal
metaphysis is interrupted by a slight bulge in the cortex.
Both irregularities indicate a supracondylar fracture.
The lateral view also shows a fracture of the distal
humerus with the distal segment angulated
posteriorly.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture.
View Case D.
Interpretation of Case C
1. Anterior fat pad: Not abnormally enlarged. It is
fairly small and it lies flat against the anterior humerus.
2. Posterior fat pad: Present. Diagnostic of a joint
effusion.
3. Anterior humeral line: Abnormal. The capitellum
is clearly posterior to the anterior humeral line. This
indicates that there is a supracondylar fracture
displacing the distal segment posteriorly or a
Salter-Harris type I fracture between the capitellum and
humerus displacing the capitellum posteriorly.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible. This is normal.
7. Hourglass sign: Present. However, again note
that the hourglass is crinkled.
8. Distal humerus: Abnormal. The metaphysis of
the distal lateral (on the right) humerus on the AP view
shows a large buckling irregularity of the cortex. On the
medial side (left), the smooth contour of the distal
metaphysis is interrupted by a slight bulge in the cortex.
Both irregularities indicate a supracondylar fracture.
The lateral view also shows a fracture of the distal
humerus with the distal segment angulated
posteriorly.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture.
View Case D.
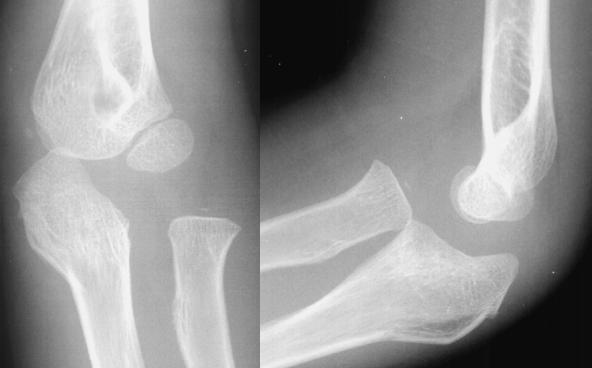
 Interpretation of Case D
1. Anterior fat pad: Difficult to see any fat pad at all.
2. Posterior fat pad: Possibly very faint. Not
definite.
3. Anterior humeral line: Normal.
4. Radial head contour: Probably normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
and internal epicondyle centers are ossified. This is
normal.
7. Hourglass sign: Present.
8. Distal humerus: Normal.
9. Olecranon/Ulna: Proximal ulna shows a fracture
inferiorly on the lateral view.
Impression: Olecranon fracture.
View Case E.
Interpretation of Case D
1. Anterior fat pad: Difficult to see any fat pad at all.
2. Posterior fat pad: Possibly very faint. Not
definite.
3. Anterior humeral line: Normal.
4. Radial head contour: Probably normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
and internal epicondyle centers are ossified. This is
normal.
7. Hourglass sign: Present.
8. Distal humerus: Normal.
9. Olecranon/Ulna: Proximal ulna shows a fracture
inferiorly on the lateral view.
Impression: Olecranon fracture.
View Case E.
 Interpretation of Case E
1. Anterior fat pad: Abnormal. Its shape is
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum and radial
head centers are ossified. This sequence is normal.
7. Hourglass sign: Absent. This indicates that the
lateral view is oblique. Such a view is not ideal.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case F.
Interpretation of Case E
1. Anterior fat pad: Abnormal. Its shape is
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum and radial
head centers are ossified. This sequence is normal.
7. Hourglass sign: Absent. This indicates that the
lateral view is oblique. Such a view is not ideal.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case F.
 Interpretation of Case F
This case consists of a lateral view only. An AP
view was taken of the forearm, but the top was cut off
through the elbow.
1. Anterior fat pad: Not able to see it.
2. Posterior fat pad: Not able to see one.
3. Anterior humeral line: Not quite perfect. The
anterior humeral line intersects the anterior third of the
capitellum. This suggests that the capitellum is
displaced posteriorly. However, since the capitellum is
nearly fully ossified, no visible fracture is evident.
4. Radial head contour: Normal.
5. Radiocapitellar line: Out of alignment. The
radius is not pointing at the capitellum, indicating a
dislocated radial head.
6. Ossification centers: Not applicable since the
elbow is nearly fully ossified.
7. Hourglass sign: Present, but not easy to see.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Obvious fracture of the ulna
shaft and possible fracture of the olecranon. Such an
obvious fracture will often dominate the radiograph.
This overshadows other findings. This pitfall of missing
the radial head dislocation is one that should be
avoided by always examining the radiocapitellar line
whenever an ulna fracture is noted.
Impression: Monteggia Injury (ulna fracture and
radial head dislocation).
View Case G.
Interpretation of Case F
This case consists of a lateral view only. An AP
view was taken of the forearm, but the top was cut off
through the elbow.
1. Anterior fat pad: Not able to see it.
2. Posterior fat pad: Not able to see one.
3. Anterior humeral line: Not quite perfect. The
anterior humeral line intersects the anterior third of the
capitellum. This suggests that the capitellum is
displaced posteriorly. However, since the capitellum is
nearly fully ossified, no visible fracture is evident.
4. Radial head contour: Normal.
5. Radiocapitellar line: Out of alignment. The
radius is not pointing at the capitellum, indicating a
dislocated radial head.
6. Ossification centers: Not applicable since the
elbow is nearly fully ossified.
7. Hourglass sign: Present, but not easy to see.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Obvious fracture of the ulna
shaft and possible fracture of the olecranon. Such an
obvious fracture will often dominate the radiograph.
This overshadows other findings. This pitfall of missing
the radial head dislocation is one that should be
avoided by always examining the radiocapitellar line
whenever an ulna fracture is noted.
Impression: Monteggia Injury (ulna fracture and
radial head dislocation).
View Case G.
 Interpretation of Case G
1. Anterior fat pad: Abnormal. It is prominent and
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: No definite posterior fat pad
visible.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
internal epicondyle, and trochlea centers are ossified.
This sequence is normal. Take a good look at the
trochlea since this ossification center is small and not
easy to see on most films. In the AP view, it is located
between the capitellum and the internal epicondyle.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case H.
Interpretation of Case G
1. Anterior fat pad: Abnormal. It is prominent and
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: No definite posterior fat pad
visible.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
internal epicondyle, and trochlea centers are ossified.
This sequence is normal. Take a good look at the
trochlea since this ossification center is small and not
easy to see on most films. In the AP view, it is located
between the capitellum and the internal epicondyle.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case H.
 Interpretation of Case H
1. Anterior fat pad: Not visible.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Not quite normal. The line
passess slightly anterior to the center of the capitellum.
4. Radial head contour: Normal on the lateral.
However, the AP view shows a knob-like radial head.
The proximal radius also appears to be bent at the
biceps tuberosity.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
and internal epicondyle (barely) centers are ossified.
This sequence is normal.
7. Hourglass sign: Present.
8. Distal humerus: Small, subtle lucency through
the distal humerus most evident on the left (medial
side). No angulation is noted on the lateral view since
the anterior humeral line bisects the capitellum.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture
and possible proximal radius fracture
View Case I.
Interpretation of Case H
1. Anterior fat pad: Not visible.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Not quite normal. The line
passess slightly anterior to the center of the capitellum.
4. Radial head contour: Normal on the lateral.
However, the AP view shows a knob-like radial head.
The proximal radius also appears to be bent at the
biceps tuberosity.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
and internal epicondyle (barely) centers are ossified.
This sequence is normal.
7. Hourglass sign: Present.
8. Distal humerus: Small, subtle lucency through
the distal humerus most evident on the left (medial
side). No angulation is noted on the lateral view since
the anterior humeral line bisects the capitellum.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Supracondylar fracture
and possible proximal radius fracture
View Case I.
 Interpretation of Case I
1. Anterior fat pad: Abnormal. It resembles a sail
(the sail sign). Hemorrhaging into the joint is pushing
the periarticular fat out of the joint.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Abnormal, indicating a
dislocated radial head. In both views, the radius is not
pointing directly at the capitellum.
6. Ossification centers: The capitellum is ossified.
There are tiny ossification sites at the radial head and
the internal epicondyle. This sequence is normal.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Distorted. Olecranon fracture.
Impression: Joint effusion. Monteggia injury.
Olecranon fracture and radial head dislocation.
View Case J.
Interpretation of Case I
1. Anterior fat pad: Abnormal. It resembles a sail
(the sail sign). Hemorrhaging into the joint is pushing
the periarticular fat out of the joint.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Abnormal, indicating a
dislocated radial head. In both views, the radius is not
pointing directly at the capitellum.
6. Ossification centers: The capitellum is ossified.
There are tiny ossification sites at the radial head and
the internal epicondyle. This sequence is normal.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Distorted. Olecranon fracture.
Impression: Joint effusion. Monteggia injury.
Olecranon fracture and radial head dislocation.
View Case J.
 Interpretation of Case J
1. Anterior fat pad: Abnormal. Prominent and
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
ossified.
7. Hourglass sign: Although the lateral view
appears to be somewhat oblique, an hourglass sign is
present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Linear lucency down the center
of the long axis of the ulna best seen on the AP view.
You may need to enlarge to image to see this.
Impression: Joint effusion. Ulna fracture.
View Case K.
Interpretation of Case J
1. Anterior fat pad: Abnormal. Prominent and
triangular. Indicates the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
ossified.
7. Hourglass sign: Although the lateral view
appears to be somewhat oblique, an hourglass sign is
present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Linear lucency down the center
of the long axis of the ulna best seen on the AP view.
You may need to enlarge to image to see this.
Impression: Joint effusion. Ulna fracture.
View Case K.
 Interpretation of Case K
1. Anterior fat pad: Abnormal. Sail sign
configuration indicating the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Not quite normal. The line
intersects the posterior portion of the capitellum.
4. Radial head contour: Possibly abnormal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum and radial
head centers are ossified. This sequence is normal.
7. Hourglass sign: Present but somewhat warped.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture
except for a possible radial head fracture.
View Case L.
Interpretation of Case K
1. Anterior fat pad: Abnormal. Sail sign
configuration indicating the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Not quite normal. The line
intersects the posterior portion of the capitellum.
4. Radial head contour: Possibly abnormal.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum and radial
head centers are ossified. This sequence is normal.
7. Hourglass sign: Present but somewhat warped.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture
except for a possible radial head fracture.
View Case L.
 Interpretation of Case L
1. Anterior fat pad: Normal. Flat and adherent to
the anterior humerus.
2. Posterior fat pad: Absent.
3. Anterior humeral line: Abnormal. The anterior
humeral line does not bisect the capitellum. This is
probably not due to displacement of the capitellum.
This is probably due to poor positioning of the lateral
view. This is an oblique view, not a true lateral.
4. Radial head contour: Abnormal. Note the
sharp angle to the radial head metaphysis seen on the
AP view, indicating a radial head fracture.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible.
7. Hourglass sign: Absent. This indicates that the
lateral view is oblique. This accounts for the abnormal
anterior humeral line.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Radial head fracture.
View Case M.
Interpretation of Case L
1. Anterior fat pad: Normal. Flat and adherent to
the anterior humerus.
2. Posterior fat pad: Absent.
3. Anterior humeral line: Abnormal. The anterior
humeral line does not bisect the capitellum. This is
probably not due to displacement of the capitellum.
This is probably due to poor positioning of the lateral
view. This is an oblique view, not a true lateral.
4. Radial head contour: Abnormal. Note the
sharp angle to the radial head metaphysis seen on the
AP view, indicating a radial head fracture.
5. Radiocapitellar line: Normal.
6. Ossification centers: Only the capitellum is
visible.
7. Hourglass sign: Absent. This indicates that the
lateral view is oblique. This accounts for the abnormal
anterior humeral line.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Radial head fracture.
View Case M.
 Interpretation of Case M
1. Anterior fat pad: Prominent, indicating a
probable joint effusion.
2. Posterior fat pad: Faint, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal. There is a small
fragment above the radial head seen on the lateral
view.
5. Radiocapitellar line: Normal.
6. Ossification centers: The elbow is nearly fully
ossified. The capitellum, radial head, internal
epicondyle, and trochlea centers are nearly fully
developed. The olecranon center is ossified. Of the
two fragments on the lateral aspect (left side) of the
distal humerus, one might be the external epicondyle
ossification center. The other is a fracture fragment.
Both may be fracture fragments. In this case, the
CRITOE sequence does not help distinguish a normal
external epicondyle from a fracture fragment since the
external epicondyle is the last to appear.
7. Hourglass sign: Present.
8. Distal humerus: There are two or three
fragments that do not represent ossification centers.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Multiple fracture
fragments.
View Case N.
Interpretation of Case M
1. Anterior fat pad: Prominent, indicating a
probable joint effusion.
2. Posterior fat pad: Faint, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal. There is a small
fragment above the radial head seen on the lateral
view.
5. Radiocapitellar line: Normal.
6. Ossification centers: The elbow is nearly fully
ossified. The capitellum, radial head, internal
epicondyle, and trochlea centers are nearly fully
developed. The olecranon center is ossified. Of the
two fragments on the lateral aspect (left side) of the
distal humerus, one might be the external epicondyle
ossification center. The other is a fracture fragment.
Both may be fracture fragments. In this case, the
CRITOE sequence does not help distinguish a normal
external epicondyle from a fracture fragment since the
external epicondyle is the last to appear.
7. Hourglass sign: Present.
8. Distal humerus: There are two or three
fragments that do not represent ossification centers.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Multiple fracture
fragments.
View Case N.
 Interpretation of Case N
1. Anterior fat pad: Prominent and triangular,
indicating the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Not applicable since this
elbow is fully ossified.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case O.
Interpretation of Case N
1. Anterior fat pad: Prominent and triangular,
indicating the presence of a joint effusion.
2. Posterior fat pad: Present, indicating a joint
effusion.
3. Anterior humeral line: Normal.
4. Radial head contour: Normal.
5. Radiocapitellar line: Normal.
6. Ossification centers: Not applicable since this
elbow is fully ossified.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. No visible fracture.
View Case O.
 Interpretation of Case O
1. Anterior fat pad: Abnormal. Prominent and
triangular indicating the presence of a joint effusion.
2. Posterior fat pad: Not visible.
3. Anterior humeral line: Normal.
4. Radial head contour: Abnormal. On the AP
view, there is a slight angle in the lateral (left side)
metaphysis of the radial head. This slight angle is an
interruption in the cortex of the radial head metaphysis.
This is only visible on the enlarged view. It is best seen
on the oblique view which is not shown here. The
oblique view of this patient is presented in Case 17 of
Volume 1.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
internal epicondyle, and olecranon centers are ossified.
The trochlea is not seen. This can be considered
abnormal, but because the trochlea is tiny, it may
already be fused to the distal humerus. This sequence
is probably within normal limits. The absence of
tenderness over the olecranon would indicate that this
ossification center is not a fracture.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Radial head fracture.
View Case P.
Interpretation of Case O
1. Anterior fat pad: Abnormal. Prominent and
triangular indicating the presence of a joint effusion.
2. Posterior fat pad: Not visible.
3. Anterior humeral line: Normal.
4. Radial head contour: Abnormal. On the AP
view, there is a slight angle in the lateral (left side)
metaphysis of the radial head. This slight angle is an
interruption in the cortex of the radial head metaphysis.
This is only visible on the enlarged view. It is best seen
on the oblique view which is not shown here. The
oblique view of this patient is presented in Case 17 of
Volume 1.
5. Radiocapitellar line: Normal.
6. Ossification centers: The capitellum, radial head,
internal epicondyle, and olecranon centers are ossified.
The trochlea is not seen. This can be considered
abnormal, but because the trochlea is tiny, it may
already be fused to the distal humerus. This sequence
is probably within normal limits. The absence of
tenderness over the olecranon would indicate that this
ossification center is not a fracture.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Normal.
Impression: Joint effusion. Radial head fracture.
View Case P.
 Interpretation of Case P
1. Anterior fat pad: Very large, indicating the
presence of a joint effusion.
2. Posterior fat pad: Probably present. A soft
tissue lucency is noted more inferiorly than the usual
position.
3. Anterior humeral line: Normal.
4. Radial head contour: The AP view of the radial
head shows a sharp angle interrupting the smooth
contour of the radial head metaphysis on the lateral
(left) side. The radial head contour on the lateral view
looks normal.
5. Radiocapitellar line: Normal in the AP view, but
slightly out of alignment in the lateral view, indicating
a slight radial head dislocation.
6. Ossification centers: Only the capitellum is
ossified.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Distorted olecranon on the AP
view indicating a fracture. The lateral view looks
normal.
Impression: Joint effusion. Monteggia injury.
Radial head fracture and dislocation. Ulna (olecranon)
fracture.
Interpretation of Case P
1. Anterior fat pad: Very large, indicating the
presence of a joint effusion.
2. Posterior fat pad: Probably present. A soft
tissue lucency is noted more inferiorly than the usual
position.
3. Anterior humeral line: Normal.
4. Radial head contour: The AP view of the radial
head shows a sharp angle interrupting the smooth
contour of the radial head metaphysis on the lateral
(left) side. The radial head contour on the lateral view
looks normal.
5. Radiocapitellar line: Normal in the AP view, but
slightly out of alignment in the lateral view, indicating
a slight radial head dislocation.
6. Ossification centers: Only the capitellum is
ossified.
7. Hourglass sign: Present.
8. Distal humerus: No irregularities seen.
9. Ulna/Olecranon: Distorted olecranon on the AP
view indicating a fracture. The lateral view looks
normal.
Impression: Joint effusion. Monteggia injury.
Radial head fracture and dislocation. Ulna (olecranon)
fracture.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page