Test Your Skill In Reading Pediatric Ankles
Radiology Cases in Pediatric Emergency Medicine
Volume 3, Case 5
Alson S. Inaba, MD
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
This case consists of 16 ankle radiograph sets.
Limited histories will be provided in most of them.
When lateral views are shown, the heel is to the left of
the image and the toes point toward the right on the
image.
Case A:
18-year old male with an inversion injury.
View Case A.
 Interpretation of Case A
AP and lateral views are displayed. The AP view
shows a fracture of the lateral cortex of the distal fibula.
The lateral view shows an oblilque fracture through the
distal fibula. The AP view shows a black crescent in
the tibia which is an artifact from poor film handling.
There is a slight irregularity of the medial metaphysis of
the distal tibia, however, the patient is not tender there.
Impression: Oblique fracture of the distal fibula.
Case B:
This is a 6-year old male who sustained an inversion
injury 6 hours prior to the ED visit. He was initially
limping, but he is now walking normally. There is
minimal tenderness of the lateral malleolus.
View Case B.
Interpretation of Case A
AP and lateral views are displayed. The AP view
shows a fracture of the lateral cortex of the distal fibula.
The lateral view shows an oblilque fracture through the
distal fibula. The AP view shows a black crescent in
the tibia which is an artifact from poor film handling.
There is a slight irregularity of the medial metaphysis of
the distal tibia, however, the patient is not tender there.
Impression: Oblique fracture of the distal fibula.
Case B:
This is a 6-year old male who sustained an inversion
injury 6 hours prior to the ED visit. He was initially
limping, but he is now walking normally. There is
minimal tenderness of the lateral malleolus.
View Case B.
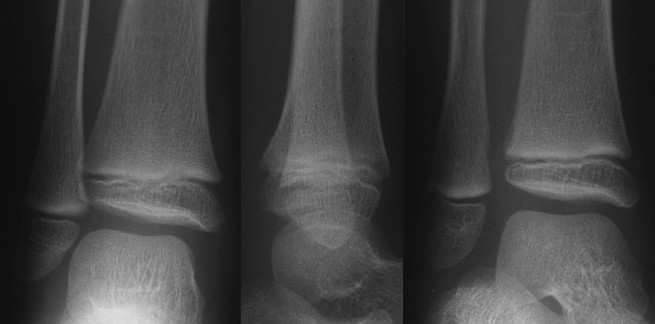 Interpretation of Case B
AP, lateral, and mortise views are displayed. There
is a small bony density contiguous with the medial
malleolus which is probably a developmental variant in
view of his tenderness over the lateral malleolus only.
This is very faint, best seen on the AP view and
posteriorly (left) on the lateral view. To see it best, turn
down the room lights and adjust the brightness and
contrast on your monitor.
Impression: Probably normal ankle. Small bony
density contiguous with the medial malleolus, probably
a developmental variant.
Case C:
This is a 14-year old male who sustained a twisting
injury playing football when he stepped into a hole. He
has tenderness over his medial malleolus and is unable
to bear weight.
View Case C.
Interpretation of Case B
AP, lateral, and mortise views are displayed. There
is a small bony density contiguous with the medial
malleolus which is probably a developmental variant in
view of his tenderness over the lateral malleolus only.
This is very faint, best seen on the AP view and
posteriorly (left) on the lateral view. To see it best, turn
down the room lights and adjust the brightness and
contrast on your monitor.
Impression: Probably normal ankle. Small bony
density contiguous with the medial malleolus, probably
a developmental variant.
Case C:
This is a 14-year old male who sustained a twisting
injury playing football when he stepped into a hole. He
has tenderness over his medial malleolus and is unable
to bear weight.
View Case C.
 Interpretation of Case C
AP and lateral views are displayed. The AP view
shows a very slight lucency above the medial malleolus.
It can be seen at the medial edge of the tibial
metaphysis just above the physis. The lateral view is
positioned such that the heel is on the left and the toes
are on the right. This lateral view shows the fracture
better along the anterior distal tibia.
Impression: Probable non-displaced medial
malleolus (tibial metaphysis) fracture.
Case D:
14-year old male with an ankle injury.
View Case D.
Interpretation of Case C
AP and lateral views are displayed. The AP view
shows a very slight lucency above the medial malleolus.
It can be seen at the medial edge of the tibial
metaphysis just above the physis. The lateral view is
positioned such that the heel is on the left and the toes
are on the right. This lateral view shows the fracture
better along the anterior distal tibia.
Impression: Probable non-displaced medial
malleolus (tibial metaphysis) fracture.
Case D:
14-year old male with an ankle injury.
View Case D.
 Interpretation of Case D
AP, mortise, and lateral views are displayed. There
is a vertical lucency through the distal tibial epiphysis
extending from the physis to the mortise joint space.
Impression: Salter Harris Type III fracture of the
distal tibia.
Case E:
This is a 10-year old male who twisted his ankle
skateboarding. He complains of pain over his lateral
malleolus. There is tenderness and moderate swelling
over the lateral malleolus.
View Case E.
Interpretation of Case D
AP, mortise, and lateral views are displayed. There
is a vertical lucency through the distal tibial epiphysis
extending from the physis to the mortise joint space.
Impression: Salter Harris Type III fracture of the
distal tibia.
Case E:
This is a 10-year old male who twisted his ankle
skateboarding. He complains of pain over his lateral
malleolus. There is tenderness and moderate swelling
over the lateral malleolus.
View Case E.
 Interpretation of Case E
AP and mortise views are shown here. There are
no definite abnormalities on this radiograph. The
lucency above the medial malleolus at the medial tibial
metaphysis does not represent a fracture since the
patient is not tender there.
Impression: Normal ankle radiographs.
However on closer examination of this patient, he is
not tender over the tip of the fibula, he is mostly tender
over the fibular physis raising the possibility of a
non-displaced Salter Harris Type I fracture through the
fibular physis. This is a clinical diagnosis, not a
radiographic diagnosis. Such injuries should be
splinted and followed clinically. For a more in-depth
review of the Salter-Harris fracture classifications, refer
to Case 18 in Volume 1.
Clinical Impression: Rule out a non-displaced Salter
Harris Type I fracture of the distal fibular physis.
Case F:
A TV set fell on the lower leg of this 18-month old.
View Case F.
Interpretation of Case E
AP and mortise views are shown here. There are
no definite abnormalities on this radiograph. The
lucency above the medial malleolus at the medial tibial
metaphysis does not represent a fracture since the
patient is not tender there.
Impression: Normal ankle radiographs.
However on closer examination of this patient, he is
not tender over the tip of the fibula, he is mostly tender
over the fibular physis raising the possibility of a
non-displaced Salter Harris Type I fracture through the
fibular physis. This is a clinical diagnosis, not a
radiographic diagnosis. Such injuries should be
splinted and followed clinically. For a more in-depth
review of the Salter-Harris fracture classifications, refer
to Case 18 in Volume 1.
Clinical Impression: Rule out a non-displaced Salter
Harris Type I fracture of the distal fibular physis.
Case F:
A TV set fell on the lower leg of this 18-month old.
View Case F.
 Interpretation of Case F.
AP and lateral views are displayed. There are
disruptions in the cortices of the distal fibular and tibial
metaphyses. These are torus fractures of the distal
fibula and tibia. There is a second fracture of the fibula
more proximal (upper portion of the image) with a
modest degree of medial angulation (i.e., angle points
to the medial side) seen best on the AP view.
Impression: Torus fractures of the fibula and tibia.
Angulated fracture of the distal fibular diaphysis.
Case G:
This is an 18-year old male with an ankle inversion
injury. He is tender over the distal aspect of the lateral
malleolus.
View Case G.
Interpretation of Case F.
AP and lateral views are displayed. There are
disruptions in the cortices of the distal fibular and tibial
metaphyses. These are torus fractures of the distal
fibula and tibia. There is a second fracture of the fibula
more proximal (upper portion of the image) with a
modest degree of medial angulation (i.e., angle points
to the medial side) seen best on the AP view.
Impression: Torus fractures of the fibula and tibia.
Angulated fracture of the distal fibular diaphysis.
Case G:
This is an 18-year old male with an ankle inversion
injury. He is tender over the distal aspect of the lateral
malleolus.
View Case G.
 Interpretation of Case G.
AP, mortise, and lateral views are displayed. There
is a small bony density adjacent to the tip of the lateral
malleolus. This could represent an avulsion fracture of
distal fibula or an accessory ossicle. Since clinically he
is tender in this area, this probably represents a small
avulsion fracture of the tip of the fibula.
Impression: Small avulsion fracture of the distal
fibula.
Case H:
This is a 23-year old male who severely twisted his
ankle. He was running and he stepped into a deep
hole.
View Case H.
Interpretation of Case G.
AP, mortise, and lateral views are displayed. There
is a small bony density adjacent to the tip of the lateral
malleolus. This could represent an avulsion fracture of
distal fibula or an accessory ossicle. Since clinically he
is tender in this area, this probably represents a small
avulsion fracture of the tip of the fibula.
Impression: Small avulsion fracture of the distal
fibula.
Case H:
This is a 23-year old male who severely twisted his
ankle. He was running and he stepped into a deep
hole.
View Case H.
 Interpretation of Case H.
AP, mortise, and lateral views are displayed. There
is an oblique, slightly displaced fracture of the distal
portion of the shaft of the fibula. There may be minimal
widening of the medial aspect of the ankle mortise. A
small avulsion fracture is noted between the dome of
the talus and the medial malleolus. This small fragment
is best seen on the AP view just inside the medial
malleolus. This may be hard to see. You may have to
enlarge the image, turn down the room lights, and
adjust the contrast and brightness on your monitor.
Impression: Oblique fracture of the distal fibula and
a small avulsion fracture which projects between the
medial malleolus and the dome of the talus.
Case I:
This is an 8-year old male who injured his ankle
while skateboarding. He has tenderness over his
medial malleolus.
View Case I.
Interpretation of Case H.
AP, mortise, and lateral views are displayed. There
is an oblique, slightly displaced fracture of the distal
portion of the shaft of the fibula. There may be minimal
widening of the medial aspect of the ankle mortise. A
small avulsion fracture is noted between the dome of
the talus and the medial malleolus. This small fragment
is best seen on the AP view just inside the medial
malleolus. This may be hard to see. You may have to
enlarge the image, turn down the room lights, and
adjust the contrast and brightness on your monitor.
Impression: Oblique fracture of the distal fibula and
a small avulsion fracture which projects between the
medial malleolus and the dome of the talus.
Case I:
This is an 8-year old male who injured his ankle
while skateboarding. He has tenderness over his
medial malleolus.
View Case I.
 Interpretation of Case I.
AP and mortise views are displayed. There is an
irregularity of the tip of the medial malleolus. This may
represent a normal developmental variant of
ossification. However, it may represent a fracture. A
comparison view of his other ankle is needed for
confirmation. Since he is tender over his medial
malleolus, one must assume that this is a fracture until
proven otherwise.
Impression: Irregularity of the tip of the medial
malleolus representing a fracture or a normal variant.
Case J:
This radiograph was copied off a 35mm slide. There
was no patient identifying information on the slide so
the patient's age and history are not available.
View Case J.
Interpretation of Case I.
AP and mortise views are displayed. There is an
irregularity of the tip of the medial malleolus. This may
represent a normal developmental variant of
ossification. However, it may represent a fracture. A
comparison view of his other ankle is needed for
confirmation. Since he is tender over his medial
malleolus, one must assume that this is a fracture until
proven otherwise.
Impression: Irregularity of the tip of the medial
malleolus representing a fracture or a normal variant.
Case J:
This radiograph was copied off a 35mm slide. There
was no patient identifying information on the slide so
the patient's age and history are not available.
View Case J.
 Interpretation of Case J.
AP, mortise, and lateral views are displayed. There
is an obvious fracture through the medial malleolus.
Note that this fracture is obvious on the mortise view,
but very subtle on the AP view. This fracture might
have been missed if a mortise view was not obtained.
Impression. Medial malleolus fracture.
Note: This is NOT a Salter-Harris type III fracture since
the fracture line does not extend into the physis (growth
plate). Salter-Harris fractures, by definition, must
involve the physis.
Case K:
This is a 17-year old male who twisted his ankle
during a soccer game. He was initially ambulatory, but
he could not bear any weight on his injured ankle the
next day. He has tenderness over the lateral aspect of
his ankle.
View Case K.
Interpretation of Case J.
AP, mortise, and lateral views are displayed. There
is an obvious fracture through the medial malleolus.
Note that this fracture is obvious on the mortise view,
but very subtle on the AP view. This fracture might
have been missed if a mortise view was not obtained.
Impression. Medial malleolus fracture.
Note: This is NOT a Salter-Harris type III fracture since
the fracture line does not extend into the physis (growth
plate). Salter-Harris fractures, by definition, must
involve the physis.
Case K:
This is a 17-year old male who twisted his ankle
during a soccer game. He was initially ambulatory, but
he could not bear any weight on his injured ankle the
next day. He has tenderness over the lateral aspect of
his ankle.
View Case K.
 Interpretation of Case K.
AP, mortise, and lateral views are displayed. There
is a fracture through the distal fibula. Although the
growth plate is almost closed, this is still technically a
Salter Harris Type I fracture through the physis. It is
radiographically visible because it is slightly displaced
as a widening of the physis. It is not easily seen on the
AP view, but it is more obvious on the mortise view.
This fracture might have been missed if a mortise view
was not obtained. A normal closure of the growth plate
will sometimes have this appearance. Comparative
views or stress views are required to confirm this
radiographically.
Impression: Probable distal fibula fracture.
Case L:
This is a 10-year old male who was struck by a car.
He has evident injuries of his head, neck, abdomen,
pelvis, and lower extremities. Only his ankle
radiographs are displayed here.
View Case L.
Interpretation of Case K.
AP, mortise, and lateral views are displayed. There
is a fracture through the distal fibula. Although the
growth plate is almost closed, this is still technically a
Salter Harris Type I fracture through the physis. It is
radiographically visible because it is slightly displaced
as a widening of the physis. It is not easily seen on the
AP view, but it is more obvious on the mortise view.
This fracture might have been missed if a mortise view
was not obtained. A normal closure of the growth plate
will sometimes have this appearance. Comparative
views or stress views are required to confirm this
radiographically.
Impression: Probable distal fibula fracture.
Case L:
This is a 10-year old male who was struck by a car.
He has evident injuries of his head, neck, abdomen,
pelvis, and lower extremities. Only his ankle
radiographs are displayed here.
View Case L.
 Interpretation of Case L.
AP, mortise, and lateral views are displayed. There
are obvious comminuted fractures of the distal one-third
of his fibula and tibia visible at the top of the image. He
may also have a medial malleolus fracture. The medial
malleolus fracture is best seen on the AP view. There
is a subtle lucency through the end of the medial
malleolus. There is an irregularity of the posterior tibia
seen best on the lateral view. This lateral view is
positioned so that the heel is to the left and the toes are
to the right. The posterior metaphysis adjacent to the
growth plate appears irregular. This is probably not a
fracture. Note that a similar finding is visible on the
lateral view in image B [Click on B].
Impression: Comminuted fractures of the distal
one-third of the fibula and tibia. Possible medial
malleolus fracture.
Case M:
This is a 3-year old female who sustained an
inversion injury while running downhill. She is limping
and has tenderness over her lateral malleolus.
View Case M.
Interpretation of Case L.
AP, mortise, and lateral views are displayed. There
are obvious comminuted fractures of the distal one-third
of his fibula and tibia visible at the top of the image. He
may also have a medial malleolus fracture. The medial
malleolus fracture is best seen on the AP view. There
is a subtle lucency through the end of the medial
malleolus. There is an irregularity of the posterior tibia
seen best on the lateral view. This lateral view is
positioned so that the heel is to the left and the toes are
to the right. The posterior metaphysis adjacent to the
growth plate appears irregular. This is probably not a
fracture. Note that a similar finding is visible on the
lateral view in image B [Click on B].
Impression: Comminuted fractures of the distal
one-third of the fibula and tibia. Possible medial
malleolus fracture.
Case M:
This is a 3-year old female who sustained an
inversion injury while running downhill. She is limping
and has tenderness over her lateral malleolus.
View Case M.
 Interpretation of Case M.
AP, mortise, and lateral views are displayed. There
are no definite bony abnormalities seen on these
radiographs. It is possible that he may have a slight
distortion of the distal fibular metaphysis (proximal to
the physis).
There is some controversy as to whether the distal
fibular epiphysis is slightly angulated or if this is a
normal appearance. According to our radiology editor,
this is not necessarily radiographically abnormal (i.e., a
normal fibula can have this appearance)..
On closer examination, her pain is mostly over the
fibular physis rather than the tip of the fibula. Because
of this, she is suspected as having a Salter Harris
Type I fracture through the fibular physis or the fracture
of the fibular metaphysis. She is placed in a splint and
is followed clinically.
Impression: Probably normal ankle radiographs.
Rule out fracture of the fibular metaphysis and/or a
Salter Harris Type I fracture of the distal fibular physis.
Case N:
This is a 13-year old male "sprained" his ankle at a
baseball game. There is obvious swelling about the
ankle joint.
View Case N.
Interpretation of Case M.
AP, mortise, and lateral views are displayed. There
are no definite bony abnormalities seen on these
radiographs. It is possible that he may have a slight
distortion of the distal fibular metaphysis (proximal to
the physis).
There is some controversy as to whether the distal
fibular epiphysis is slightly angulated or if this is a
normal appearance. According to our radiology editor,
this is not necessarily radiographically abnormal (i.e., a
normal fibula can have this appearance)..
On closer examination, her pain is mostly over the
fibular physis rather than the tip of the fibula. Because
of this, she is suspected as having a Salter Harris
Type I fracture through the fibular physis or the fracture
of the fibular metaphysis. She is placed in a splint and
is followed clinically.
Impression: Probably normal ankle radiographs.
Rule out fracture of the fibular metaphysis and/or a
Salter Harris Type I fracture of the distal fibular physis.
Case N:
This is a 13-year old male "sprained" his ankle at a
baseball game. There is obvious swelling about the
ankle joint.
View Case N.
 Interpretation of Case N.
AP, mortise, and lateral views are displayed. There
is a vertical lucency through the distal tibial epiphysis
extending from the ankle joint to the tibial physis. It
does not appear to extend into the metaphysis.
Impression: Salter Harris Type III fracture of the
distal tibia.
Case O:
This is a 9-year old female who fell off a second
floor balcony at school, landing on her feet.
View Case O.
Interpretation of Case N.
AP, mortise, and lateral views are displayed. There
is a vertical lucency through the distal tibial epiphysis
extending from the ankle joint to the tibial physis. It
does not appear to extend into the metaphysis.
Impression: Salter Harris Type III fracture of the
distal tibia.
Case O:
This is a 9-year old female who fell off a second
floor balcony at school, landing on her feet.
View Case O.
 Interpretation of Case O.
AP, mortise, and lateral views are displayed. The
lateral view also includes her foot. There are multiple
lucencies evident in her calcaneus. The tibial physis
does not appear to be widened or compressed. There
are no definite bony abnormalities of the ankle.
However, in addition to being tender over her foot, she
is also tender over her medial malleolus. The
mechanism of injury suggests the possibility of a Salter
Harris Type V fracture of the distal tibial physis. This is
often not a radiographic diagnosis, but rather a clinical
one based on examination findings and the mechanism
of injury. This type of injury may cause a growth arrest
in a portion of the growth plate causing a valgus or
varus deformity.
Impression: Multiple calcaneal fractures. Rule out
Salter Harris Type V fracture of the distal tibia.
Case P:
This is a 23-year old female college student who
twisted her ankle while jogging down a hill. She has
swelling and tenderness over her lateral malleolus.
View Case P.
Interpretation of Case O.
AP, mortise, and lateral views are displayed. The
lateral view also includes her foot. There are multiple
lucencies evident in her calcaneus. The tibial physis
does not appear to be widened or compressed. There
are no definite bony abnormalities of the ankle.
However, in addition to being tender over her foot, she
is also tender over her medial malleolus. The
mechanism of injury suggests the possibility of a Salter
Harris Type V fracture of the distal tibial physis. This is
often not a radiographic diagnosis, but rather a clinical
one based on examination findings and the mechanism
of injury. This type of injury may cause a growth arrest
in a portion of the growth plate causing a valgus or
varus deformity.
Impression: Multiple calcaneal fractures. Rule out
Salter Harris Type V fracture of the distal tibia.
Case P:
This is a 23-year old female college student who
twisted her ankle while jogging down a hill. She has
swelling and tenderness over her lateral malleolus.
View Case P.
 Interpretation of Case P.
AP, mortise, and lateral views are displayed. There
is an oblique fracture through the posterolateral aspect
of the lateral malleolus. This fracture has occurred
through the fused growth plate which remains weaker
than the surrounding bone for the next several years
following closure. The distal fibular physis usually fuses
by age 20 years and the distal tibial physis usually
fuses by age 18 years.
Impression: Lateral malleolus fracture.
Interpretation of Case P.
AP, mortise, and lateral views are displayed. There
is an oblique fracture through the posterolateral aspect
of the lateral malleolus. This fracture has occurred
through the fused growth plate which remains weaker
than the surrounding bone for the next several years
following closure. The distal fibular physis usually fuses
by age 20 years and the distal tibial physis usually
fuses by age 18 years.
Impression: Lateral malleolus fracture.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page