Lethargy and Vomiting Following Child Abuse
Radiology Cases in Pediatric Emergency Medicine
Volume 5, Case 10
Loren G. Yamamoto, MD, MPH
Kapiolani Medical Center For Women And Children
University of Hawaii John A. Burns School of Medicine
This is a 7 month old female who presents to the
emergency department with a chief complaint of a
growing lump on the side of her head. A cousin who
was baby sitting the infant six days ago had placed her
on a couch. The infant fell off the couch. The infant's
grandmother was in the home at the time. The infant
cried right away. There was no loss of consciousness
or drowsiness noted. Two days later (four days ago),
mother noted a lump developing on the right side of the
infant's head. Since then, mother has noted that the
lump has become larger and the lump feels like a large
soft spot in her head. There is no history of vomiting or
other trauma.
Exam: VS T37.5 (rectal), P140, R36, BP 75/40,
weight 5th percentile for age, height 25th percentile for
age. She is alert and active in no distress. Anterior
fontanelle flat. A 10 cm region of swelling is noted over
the right parietal region raised about 2 to 3 cm. The
swelling is soft. PERRL, red reflex present bilaterally.
Fundi difficult to view. TM's no blood. Nose clear. Oral
clear, moist. Neck non-tender, supple. Heart regular
without murmurs. Lungs clear. Trunk without bruising.
Abdomen soft, flat, bowel sounds active. No abdominal
tenderness or masses. No hernias. Normal genitalia.
Extremities without swelling, deformity, or bruising.
Tone good. Uses all extremities well.
A skull series is obtained.
View skull series.
 Clinically, this infant appears to have a subgaleal
hematoma. These usually are brought to medical
attention several days after sustaining an underlying
skull fracture. The presentation is often not immediate
since the hemorrhage from the fracture forms a tight
and palpably rigid swelling under the aponeurosis of
Galen. As blood from the hematoma is resorbed, the
swelling softens. This "soft spot" on the infant's head is
then noted by parents, often prompting a visit to a
physician. In most instances, there are no
complications, since several days have elapsed since
the head trauma without the infant exhibiting any signs
or symptoms of brain injury. Radiographs of the skull
would most often not alter one's clinical approach
except in a case such as this.
This skull series shows extensive fractures of the
right parietal skull. One would expect to see a simple
linear fracture in this region if the trauma were
accidental. Additionally, there are extensive fractures
over the occipital skull and the contralateral parietal
skull as well. A simple fall off a couch could not
possibly account for all these fractures. Child abuse is
likely. A CT scan of the brain is performed.
View CT scan.
Clinically, this infant appears to have a subgaleal
hematoma. These usually are brought to medical
attention several days after sustaining an underlying
skull fracture. The presentation is often not immediate
since the hemorrhage from the fracture forms a tight
and palpably rigid swelling under the aponeurosis of
Galen. As blood from the hematoma is resorbed, the
swelling softens. This "soft spot" on the infant's head is
then noted by parents, often prompting a visit to a
physician. In most instances, there are no
complications, since several days have elapsed since
the head trauma without the infant exhibiting any signs
or symptoms of brain injury. Radiographs of the skull
would most often not alter one's clinical approach
except in a case such as this.
This skull series shows extensive fractures of the
right parietal skull. One would expect to see a simple
linear fracture in this region if the trauma were
accidental. Additionally, there are extensive fractures
over the occipital skull and the contralateral parietal
skull as well. A simple fall off a couch could not
possibly account for all these fractures. Child abuse is
likely. A CT scan of the brain is performed.
View CT scan.
 This high CT scan cut shows a bone window on the
left and a brain window on the right. The open anterior
fontanelle is noted at the top of the both images. The
large right parietal scalp swelling (subgaleal hematoma)
is noted. The bone window on the left shows a large
right parietal fracture. A smaller left parietal fracture is
also evident. The coronal sutures are visible. There
are several lucencies in the occiput. Two of these are
the lambdoidal sutures while the others are occipital
fractures. The brain is normal. Lower cuts do not
demonstrate cerebral hemorrhages or edema. The
posterior interhemispheric subdural hematoma is not
evident on the lower cuts. This finding would be
indicative of shaken infant syndrome as noted on Case
1 of Volume 1.
A skeletal survey is obtained.
View skeletal survey.
This high CT scan cut shows a bone window on the
left and a brain window on the right. The open anterior
fontanelle is noted at the top of the both images. The
large right parietal scalp swelling (subgaleal hematoma)
is noted. The bone window on the left shows a large
right parietal fracture. A smaller left parietal fracture is
also evident. The coronal sutures are visible. There
are several lucencies in the occiput. Two of these are
the lambdoidal sutures while the others are occipital
fractures. The brain is normal. Lower cuts do not
demonstrate cerebral hemorrhages or edema. The
posterior interhemispheric subdural hematoma is not
evident on the lower cuts. This finding would be
indicative of shaken infant syndrome as noted on Case
1 of Volume 1.
A skeletal survey is obtained.
View skeletal survey.
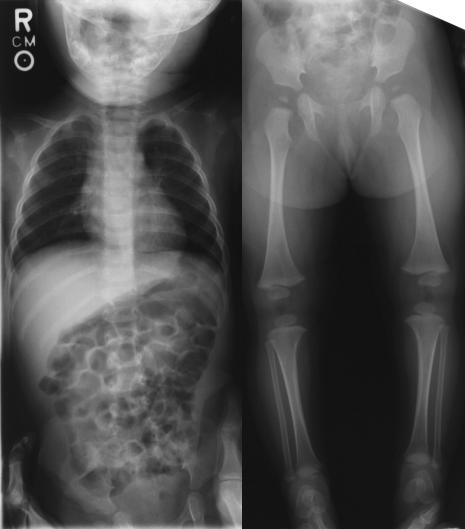 No other fractures are identified on this skeletal
survey. The upper extremities are not shown here.
They are negative for fractures as well.
Because of the likelihood of child abuse and the
potential for repeated inflicted head trauma, the infant
is hospitalized and the child protective service is
notified. During hospitalization, this infant does well.
There is good weight gain and her neurological function
and developmental evaluation are normal. A retina
exam performed by an ophthalmologist is negative for
hemorrhages.
On hospital day three, she is noted to be less active
than she has been and she vomits three times.
Abdominal examination is negative. She vomits again
and is noted to be lethargic. A nasogastric tube is
placed. A repeat CT scan is obtained to rule out a
hemorrhage. The repeat CT scan fails to find any brain
abnormalities. The skull fractures and scalp swelling
are unchanged.
Develop a differential diagnosis at this point and a
diagnostic plan. An IV is started. Laboratory studies
are drawn and she is started on IV fluids at a moderate
rate.
An abdominal series is ordered as part of her
evaluation.
View abdominal series.
No other fractures are identified on this skeletal
survey. The upper extremities are not shown here.
They are negative for fractures as well.
Because of the likelihood of child abuse and the
potential for repeated inflicted head trauma, the infant
is hospitalized and the child protective service is
notified. During hospitalization, this infant does well.
There is good weight gain and her neurological function
and developmental evaluation are normal. A retina
exam performed by an ophthalmologist is negative for
hemorrhages.
On hospital day three, she is noted to be less active
than she has been and she vomits three times.
Abdominal examination is negative. She vomits again
and is noted to be lethargic. A nasogastric tube is
placed. A repeat CT scan is obtained to rule out a
hemorrhage. The repeat CT scan fails to find any brain
abnormalities. The skull fractures and scalp swelling
are unchanged.
Develop a differential diagnosis at this point and a
diagnostic plan. An IV is started. Laboratory studies
are drawn and she is started on IV fluids at a moderate
rate.
An abdominal series is ordered as part of her
evaluation.
View abdominal series.
 The supine view is on the left and the upright view is
on the right. Is this abdominal series helpful? How
does it affect the differential diagnosis? What should
be done at this point?
This abdominal series shows a paucity of bowel gas.
An NG tube is in the stomach. Is this pattern consistent
with an ileus or a bowel obstruction? Using the criteria
described in Case 18 of Volume 3, Test Your Skill In
Distinguishing Obstruction From Ileus, the following
should be evaluated:
1. Gas distribution: There is a generalized paucity
of bowel gas and it is not distributed well.
2. Bowel dilation: This is difficult to comment on
since there is not much bowel gas visible.
3. Air-fluid levels: There are several air fluid levels
in the left upper quadrant.
4. Orderliness: The supine view does not show a
"bag of popcorn" type gas pattern. Nor does it show a
"bag of sausages" pattern since there is not much gas
here at all.
The paucity of gas is quite remarkable and
associated with several air-fluid levels, this is highly
suspicious of a bowel obstruction. Additionally, as
noted in Case 18 of Volume 3, such a "gasless" (or at
least a paucity of gas) bowel obstruction in a young
child, is highly suggestive of intussusception.
The right upper quadrant shows a hint of a mass or
a "target sign". As described in Case 2 of Volume 1
(The Stomach Flu? - The Target, Crescent, and Absent
Liver Edge Signs), this sign is a faint subtle target-like
(doughnut shaped) finding in the right upper quadrant.
The presence of this sign is highly indicative of
intussusception.
This infant actually developed an intussusception
during a hospitalization for child abuse. Note that on
her admission skeletal survey, her abdominal
radiograph shows a normal bowel gas pattern. In
retrospect, her clinical presentation of vomiting and
lethargy is highly suggestive of intussusception, yet
because she was hospitalized for head trauma and
child abuse, the diagnosis of intussusception may not
be considered as a likely possibility. It's as if
hospitalization for an unrelated problem somehow
renders inpatients an "immunity" against other medical
conditions. True, it is less likely to have two diagnoses
to explain a patient's clinical findings, however, no rule
in medicine guarantees a single etiology for all clinical
findings. Avoid this pitfall by keeping an open mind
when evaluating new findings in hospitalized patients.
A barium enema confirmed the intussusception. It
could not be reduced. She underwent a surgical
reduction of the intussusception. There were no
surgical findings to suggest that the intussusception
was related to child abuse in any way. She recovered
well and was discharged to foster care.
The supine view is on the left and the upright view is
on the right. Is this abdominal series helpful? How
does it affect the differential diagnosis? What should
be done at this point?
This abdominal series shows a paucity of bowel gas.
An NG tube is in the stomach. Is this pattern consistent
with an ileus or a bowel obstruction? Using the criteria
described in Case 18 of Volume 3, Test Your Skill In
Distinguishing Obstruction From Ileus, the following
should be evaluated:
1. Gas distribution: There is a generalized paucity
of bowel gas and it is not distributed well.
2. Bowel dilation: This is difficult to comment on
since there is not much bowel gas visible.
3. Air-fluid levels: There are several air fluid levels
in the left upper quadrant.
4. Orderliness: The supine view does not show a
"bag of popcorn" type gas pattern. Nor does it show a
"bag of sausages" pattern since there is not much gas
here at all.
The paucity of gas is quite remarkable and
associated with several air-fluid levels, this is highly
suspicious of a bowel obstruction. Additionally, as
noted in Case 18 of Volume 3, such a "gasless" (or at
least a paucity of gas) bowel obstruction in a young
child, is highly suggestive of intussusception.
The right upper quadrant shows a hint of a mass or
a "target sign". As described in Case 2 of Volume 1
(The Stomach Flu? - The Target, Crescent, and Absent
Liver Edge Signs), this sign is a faint subtle target-like
(doughnut shaped) finding in the right upper quadrant.
The presence of this sign is highly indicative of
intussusception.
This infant actually developed an intussusception
during a hospitalization for child abuse. Note that on
her admission skeletal survey, her abdominal
radiograph shows a normal bowel gas pattern. In
retrospect, her clinical presentation of vomiting and
lethargy is highly suggestive of intussusception, yet
because she was hospitalized for head trauma and
child abuse, the diagnosis of intussusception may not
be considered as a likely possibility. It's as if
hospitalization for an unrelated problem somehow
renders inpatients an "immunity" against other medical
conditions. True, it is less likely to have two diagnoses
to explain a patient's clinical findings, however, no rule
in medicine guarantees a single etiology for all clinical
findings. Avoid this pitfall by keeping an open mind
when evaluating new findings in hospitalized patients.
A barium enema confirmed the intussusception. It
could not be reduced. She underwent a surgical
reduction of the intussusception. There were no
surgical findings to suggest that the intussusception
was related to child abuse in any way. She recovered
well and was discharged to foster care.
Return to Radiology Cases In Ped Emerg Med Case Selection Page
Return to Univ. Hawaii Dept. Pediatrics Home Page